
# Weight loss drugs
Introduction
It’s a miracle! The holy grail of weight loss has been discovered! For many people, the advent of weight loss medications such as Wegovy/Ozempic and Mounjaro is the stuff of dreams. Years of struggle and self-recrimination have been replaced by substantial and relatively effortless weight loss. And note this: while there’s no shortage of scary side effect clickbait, actually, serious side effects are rare and some are more a result of rapid weight loss than from the drugs themselves. There is also some rather exciting data supporting several benefits beyond those for type 2 diabetes and weight loss. In mid-2026, half a million Australians are prescribed either Ozempic, Wegovy or Mounjaro, either for weight management or diabetes control. However, there are a couple of hurdles. Firstly, except in limited circumstances, they’re not subsidised for weight loss (and they don’t come cheaply). Also, if you stop taking them, your appetite quickly returns and weight is regained. Like anything new and noteworthy, misinformation abounds, so here we sift fact from fiction and look at what these drugs can achieve. We won’t discuss optimal nutrition during weight loss, or forestalling weight regain should you discontinue. These are important topics, relevant to anyone who loses substantial weight by any means, so we’ll save that for another day.
The epic quest for weight loss
Products aimed at circumventing the tiresome business of exercising long-term and rigorous self-restraint to manage body weight have been big business for over a century. For a long time, stimulants like amphetamines were the main game (though a shout out to tapeworm pills please); in the 1990s, anti-cannabis-type appetite suppressants had a moment (but also had anti-cannabis type negative effects on mental health); and, in the early 2000s, fat absorption blockers like Orlistat garnered great excitement (though were stymied by the leaky stool issue). But until about 15 years ago, other than surgery, nothing worked very well and the side effects ranged from unpleasant to deadly. Then a new class of drugs, known as GLP-1 receptor agonists (GLP-1 RAs) appeared.
GLP-1 receptor agonists…please explain?
These new drugs are best thought of as hyper-powered analogues for two hormones secreted naturally after eating, namely, glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), collectively called incretins.
GLP-1:
Secreted in the lower small intestine and colon
Secretion stimulated by carbohydrates and fats
GIP
Secreted in the upper small intestine
Secretion stimulated by glucose and fats
To briefly introduce the main players: Ozempic and Wegovy are brand names for semaglutide, an agonist of GLP-1 receptors only. Mounjaro and Zepbound are brand names for tirzepatide, a “twincretin” agonist of GIP and GLP-1 receptors. Tirzepatide’s modes of action are outlined below.
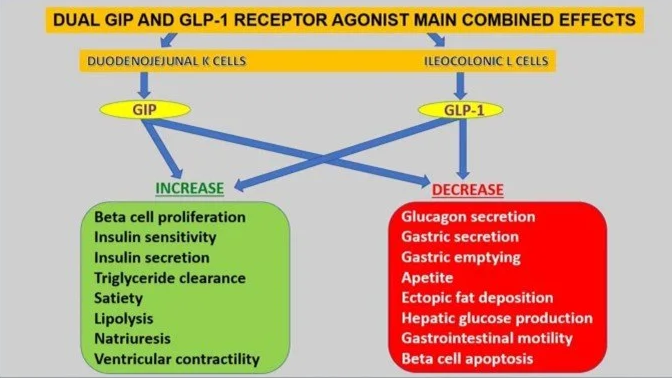
Actions of the dual incretin agonist tirzepatide. Fisman and Tenenbaum (2021). (Ref)
Bariatric surgery
Before GLP-1 RAs, bariatric surgery was the most effective treatment for obesity, producing radical weight loss; longer life expectancy and enhanced quality of life. (Ref, Ref) As the Swedish Obesity Surgery study shows, weight loss is dramatic and usually substantially sustained. This sets surgery apart from all other weight-loss approaches.
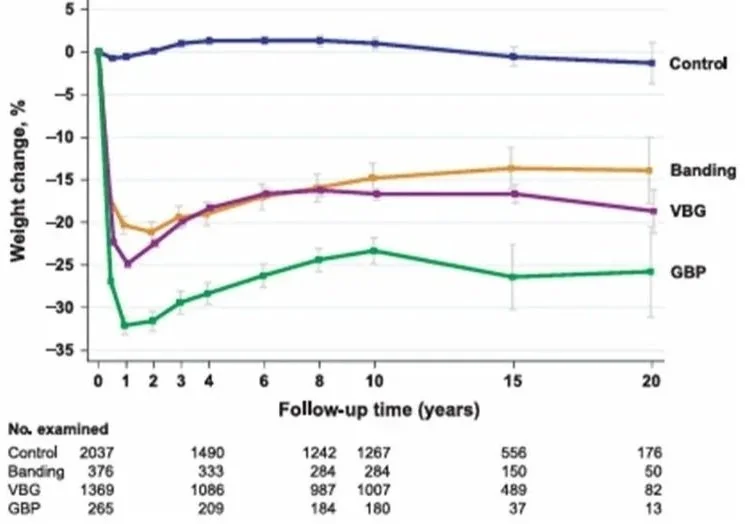
Weight loss results from the Swedish Obesity Surgery study. VBG: vertical banded gastroplasty; GBP: gastric bypass (a.k.a RYGB). Bars show 95% confidence intervals. Source: Sjöström et al (2012). (Ref)
Interestingly, calorie reductions after bariatric surgery, especially Roux-en-Y gastric bypass (RYGB), are commonly more than changes to gastrointestinal anatomy would predict, with brain changes also contributing. Post-operative magnetic resonance imaging shows reduced brain activation in dopamine-driven brain reward centres, particularly in response to hyper-palatable foods*, which are also, inevitably, calorie dense. While it’s not universally accepted as a condition, food addiction is a useful way to conceptualise the common compulsion to eat hyper-palatable foods beyond health and even beyond pleasure. So, bariatric surgery results in both a reduction in the volume of food consumed and lowered energy density of the food that is eaten.
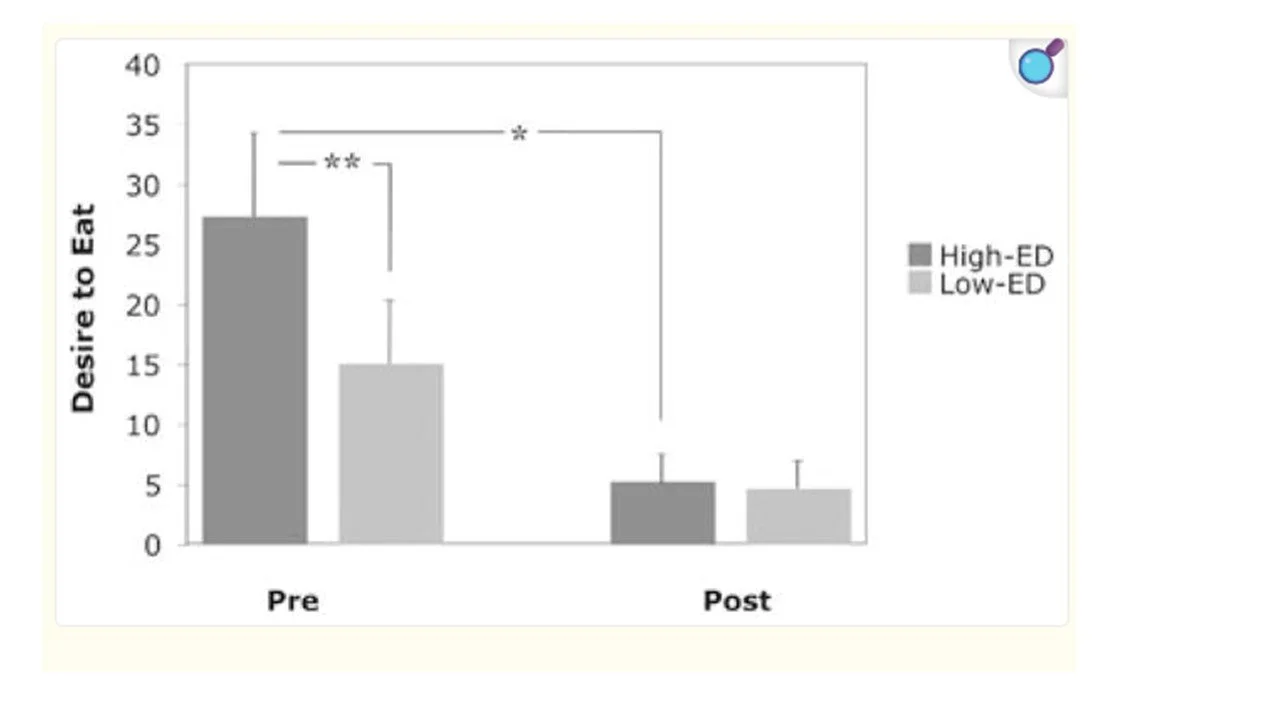
The difference between the desire to eat following exposure to high-energy dense relative to low-energy dense foods pre- and post-surgery. Source: Ochner at al (2011). (Ref)
It’s understood that reduced desire for high calorie food arises from higher GLP-1 secretion in the gut, with support for this theory lying in the fact that the inter-individual magnitude of GLP1 increases in post-surgical blood tests predict long-term post-surgical weight loss.# (Ref, Ref, Ref)
These findings have ramifications for GLP-1 RAs and, beyond this, into broader addiction research. (Ref, Ref, Ref)
*this is a whole field of study in itself, but red flags for hyper-palatable foods are two or more of the following in combination: high sugar, high fat, high salt and high starch, along with low fibre. These foods are not synonymous with ultra-processed foods (UPFs) but there’s a lot of overlap.
#Surgical or pharmacological enhancement of GLP-1 signaling reliably reduces hunger in people that generally have a history of “failure of willpower” in this area. Surely this demonstrates that body weight regulation is governed to a large extent by physiology and that weight struggles are not a sign of inferior self-control? We now accept this framing for conditions like depression and anxiety and wouldn’t suggest that merely wherewithal was lacking. Likewise, to suggest the same for obesity (or that GLP-1 drugs are cheating), is ignorant and stigmatising – and you’re better than that. (Ref)
The evolution of GLP-1 RAs
The chart below shows that GLP-1 RAs have now been around for over 20 years, providing a substantial body of long-term data. However, for most of their history, they were generally used at lower doses in diabetic patients. For higher doses, especially in non-diabetics, we have to wait until 2021 for official data. In addition, GIP inclusion is relatively recent, with tirzepatide the first to include it and only launched in 2022.
| Generic GLP-1 RA name | Brand name | Manufacturer | Indication | US launch |
|---|---|---|---|---|
| Exenatide | Byetta | Astra Zeneca | T2DM | 2005 |
| Exenatide | Bydureon BCise | Astra Zeneca | T2DM | 2012 |
| Liraglutide | Victoza | Novo Nordisk | T2DM | 2010 |
| Liraglutide | Saxenda | Novo Nordisk | T2DM | 2014 |
| Dulaglutide | Trulicity | Eli Lilly | T2DM | 2014 |
| Semaglutide | Ozempic | Novo Nordisk | T2DM | 2017 |
| Semaglutide | Rybelsus | Novo Nordisk | T2DM | 2019 |
| Semaglutide | Wegovy | Novo Nordisk | Weight | 2021 |
| Tirzepatide | Mounjaro | Eli Lilly | T2DM | 2022 |
| Tirzepatide | Zepbound | Eli Lilly | Weight | 2023 |
| Retatrutide | No brand yet | Eli Lilly | Weight | Not yet approved |
T2DM: Type 2 diabetes mellitus
Early on in their history as a diabetes medication, the effect of GLP-1 RAs on weight loss were noted. In particular, that they dramatically dampened hedonistic hunger (the brain-based yearning for hyper-palatable food we’ve already encountered), sometimes called “food noise. Clinical trials were conducted and versions specifically indicated for weight loss were launched. The inclusion of GIP was found to enhance their efficacy both for diabetes treatment and for weight loss and reduced side effects. The newest versions also include glucagon, which increases metabolic rate and reduces hypoglycaemic events. (Ref)
These medications, as receptor agonists, bind to GLP-1 and/or GIP receptors, triggering responses similar, but much larger, to those produced by naturally occurring incretins. Normally, endogenous incretins act only for a few minutes before being rapidly broken down but newer synthetic versions resist degradation, greatly prolonging their activity. The half-lives of semaglutide and tirzepatide are seven and five days, respectively. (Ref, Ref, Ref)
The Therapeutic Goods Association (TGA) has approved a number of GLP-1RAs. Key current arrangements under the pharmaceutical benefits scheme (PBS) are below.
| Product | TGA approvals | Monthly cost |
|---|---|---|
| Mounjaro (tirzepatide) | T2DM, weight management, and moderate-to-severe obstructive sleep apnoea. | Starting dose ~$395 out of pocket. No PBS subsidy. |
| Ozempic (semaglutide) | T2DM only. Use for weight loss is off-label and restricted. | $32 under the PBS for diabetes / $134 for weight loss out of pocket |
| Wegovy (semaglutide) | Weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with comorbidities, and adolescents 12+ with obesity. Also approved for cardiovascular risk reduction. | $350-460 out of pocket. In March 2026, the PBS undertook to subsidise Wegovy for patients who had heart disease and were clinically obese, under parameters defined by the PBS. |
Wegovy is the same molecule as Ozempic but in a higher dose formulation; and overseas Mounjaro is marketed as Zepbound for weight loss. Source: PBS (2026).
How much weight do people lose?
The STEP and SURMOUNT double-blind placebo controlled trials demonstrated the effectiveness of semaglutide and tirzepatide for weight loss, with tirzepatide more effective for both weight loss and lowering HbA1c at the doses tested. (Ref, Ref, Ref)
If you look back at the bariatric surgery chart, average RYGB weight loss was 25%. In comparison, tirzepatide achieved average losses at the highest dose of 21%.
| Trial | Subjects | Dose & duration | Average weight loss |
|---|---|---|---|
| STEP Phase 3 semaglutide | N = 1961 adults; BMI >30; without diabetes. | 2.4 mg/wk semaglutide or placebo, plus lifestyle intervention, for 68 weeks. | Semaglutide: -14.9% (-15.3 kg); Placebo: -2.4% (-2.6 kg) |
| SURMOUNT: Phase 3 tirzepatide | N =2539 adults; BMI >30; without diabetes. | 5 mg, 10 mg, or 15 mg tirzepatide weekly or placebo for 72 weeks, including a 20w dose-escalation. | Tirzepatide 5 mg: -15%; 10 mg: -19.5%; 15 mg: -20.9%; Placebo: -3.1% |
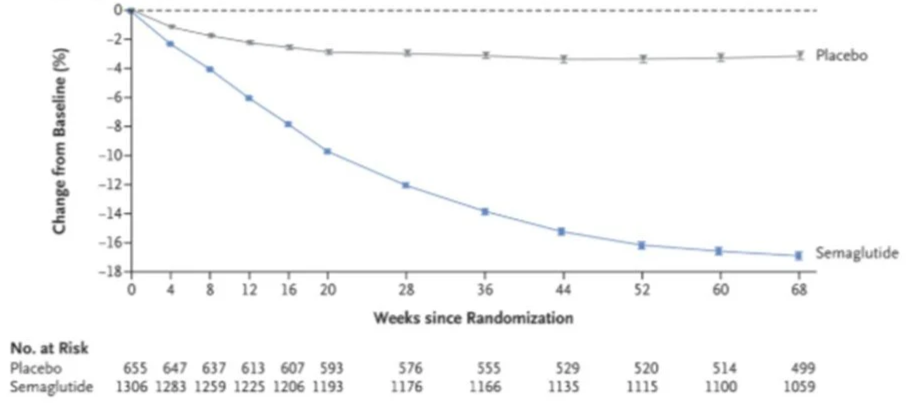
STEP Phase III: Weight loss with semaglutide compared to placebo over 68 weeks. Wilding et al (2021). (Ref)
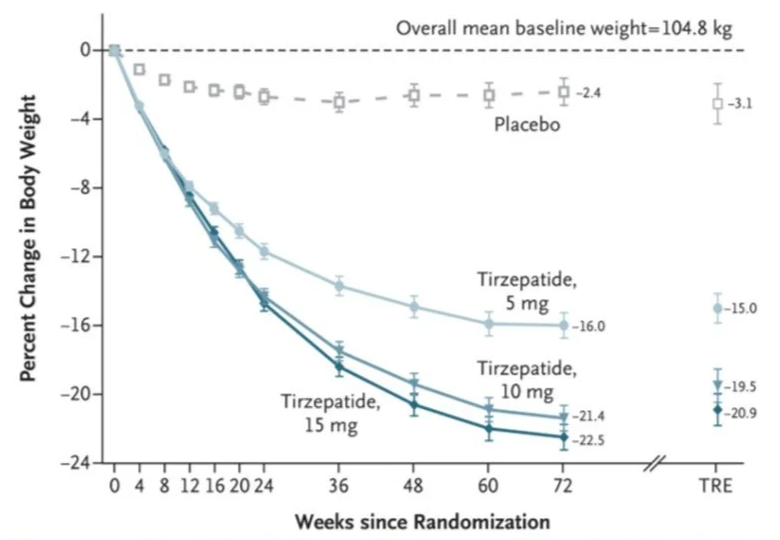
SURMOUNT Phase III: Weight change with three doses of tirzepatide compared to placebo over 72 weeks. Jastreboff et al (2022). (Ref)
Benefits beyond weight loss
Reduced weight alone reduces risk of cardiovascular disease, kidney disease, T2DM, several cancers and liver disease. However, evidence suggests GLP-1 RAs exert beneficials beyond those expected from weight loss, via receptors in the cardiovascular system, immune system and brain. Here the evidence for heart disease is the most well established. (Ref, Ref)
Postulated GLP-1 RA actions in the body.
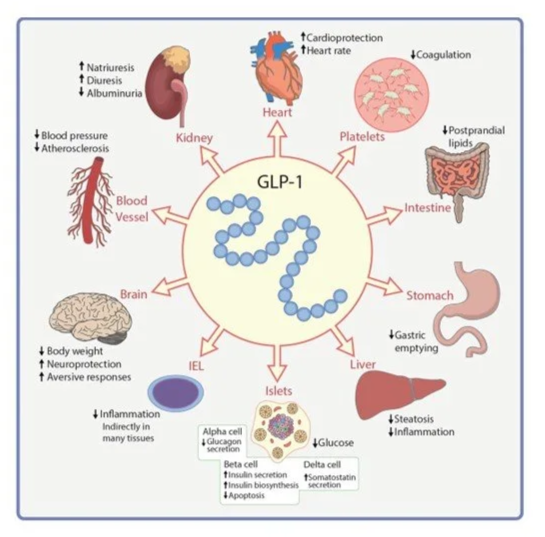
Source: Drucker and Holst (2023). (Ref)
Cardiovascular Health
In the cardiovascular system, GLP-1 reduces blood pressure, improves cholesterol, and reduces cardiovascular inflammation. Hence, it’s not surprising that GLP analogues reduce major cardiovascular events in people with and without type 2 diabetes, including death, myocardial infarction and stroke. (Ref, Ref)
In addition, GIP receptors in the blood vessel lining may suggest GIP has an anti-inflammatory effect to suppress atherosclerosis. This is currently the subject of a tirzepatide clinical trial. (Ref)
You can see cardiovascular events fell as tirzepatide dose increased in the SURMOUNT data table further on. Further research has established the benefits of GLP-1 RAs, such that it is now an indicated use of Wegovy under the PBS.
It is well established that cardiovascular disease is a key contributor to dementia risk. (Ref, Ref) Dementia and heart disease are the two top causes of death in Australia, and both also cause significant disability, hence this is very encouraging data. (Ref)
Immune system and cancer
GLP-1 analogues appear to reduce inflammation in the heart, pancreas, blood vessels, kidney, lung and brain. (Ref)
With an effect on the immune system, you might speculate as to their effect on cancer. Obesity itself is associated with 13 types of cancer, which account for some 40% of annual US cancer diagnoses. A US retrospective cohort study comparing >40 thousand subjects taking GLP-1RAs for weight management to an equivalent number of controls, found GLP-1RAs were associated with 17% fewer cancer incidences. In particular endometrial (-14%), meningioma (-31%), and ovarian cancer (-17%) were reduced. Kidney cancer however trended higher. (Ref)
Risk of 14 Cancers in subjects receiving GLP-1RAs compared with control subjects is charted below. For more on interpreting these graphs see here but for now know that dots to the left of the vertical line denote fewer cancer cases with GLP-1 RAs and that statistical significance was reached where the line doesn’t cross the vertical.
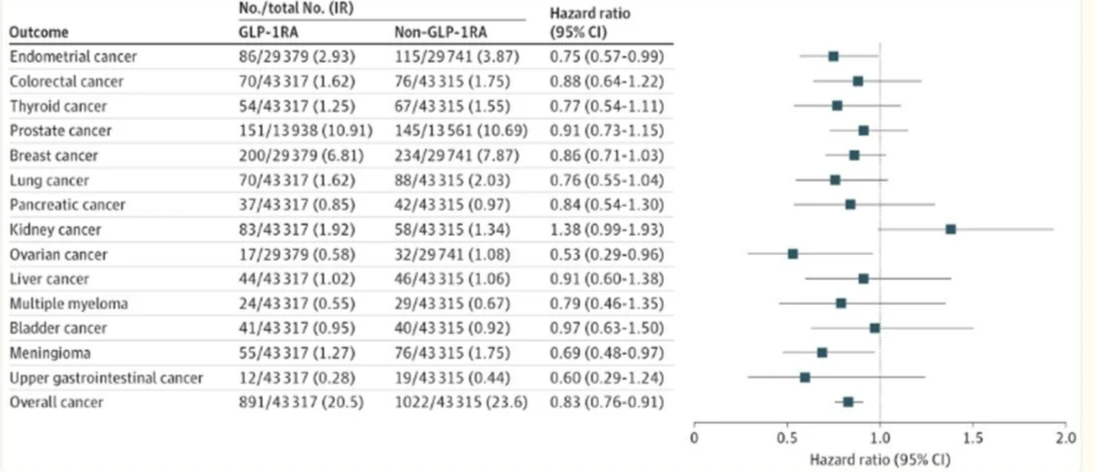
Hazard ratios with 95% confidence intervals showing the risk of cancer with GLP-1 RAs. Source: Dai et al (2025). (Ref)
Thyroid Cancer
Thyroid cancer warrants further discussion.
The study above didn’t find an increase in thyroid cancer, in fact in trended lower. However, rodent studies indicate GLP-1RAs increase thyroid cancer risk and there is a boxed warning on medication specifically for medullary thyroid cancer (MTC). (Ref) Moreover, insulin resistance, as occurs in diabetes and pre-diabetes, is also associated with increased thyroid cancer, one study finding 216% increased risk. (Ref, Ref) And GLP1-RAs appear to further increase this risk. A French cross sectional study found use of GLP-1 RAs for diabetes, compared to alternative therapy, was linked to a 58% increased risk of thyroid cancer, including a 78% increased risk of MTC. (Ref)
Absolute risk however is very low. Australian data reports ~14 in 100,000 people are diagnosed with thyroid cancer annually and, <1 person/100,000 is diagnosed with MTC. And even with a diagnosis, average survival is 97% after 5 years. (Ref)
Hence GLP1-RAs tend only to be contra-indicated at people with a history or genetic risk of thyroid cancer.
Addiction
This part is very interesting. The effects of GLP-1 in the brain extend beyond appetite control, with the same reduction in the dopamine-driven urge to eat hyper-palatable foods, also apparently curbing other reward-driven behaviors. (Ref) For instance, reduced urge to drink alcohol have been clinically observed, as have nicotine cravings. (Ref) Studies on other addictive substances show some positive signs but results are mixed and at an early stage. (Ref)
Okay, what about other downsides?
While there’s a tendency to extrapolate from celebrity anecdote and other dubious sources of information, serious adverse consequences are rare.
While high dose GLP-1 RA use for weight management has only been practised in earnest for five years, the sheer size of the population using higher dose GLP-1 RAs (both with and without GIP and with and without diabetes) over this period has still demonstrated relatively few material side effects, adding support to the safety profile of GLP-1 RAs.
The table below is extensive but important. It details the proportion of subjects who experienced side effects in the SURMOUNT tirzepatide trial. Of course, we’re interested in effects where subjects receiving the drug were significantly more affected than those receiving placebo. Of course, it only covers 72 weeks so is indicative only. Further studies have assessed many of these factors further.
SURMOUNT Data Table
| Tirzepatide 5 mg | Tirzepatide 10 mg | Tirzepatide 15 mg | Placebo | |
|---|---|---|---|---|
| (N=630) | (N=636) | (N=630) | (N=643) | |
| % | % | % | ||
| Death | 0.6 | 0.3 | 0.2 | 0.6 |
| Nausea | 24.6 | 33.3 | 31 | 9.5 |
| Diarrhea | 18.7 | 21.2 | 23 | 7.3 |
| Covid-19 | 14.9 | 15.4 | 13 | 14 |
| Constipation | 16.8 | 17.1 | 11.7 | 5.8 |
| Dyspepsia | 8.9 | 9.7 | 11.3 | 4.2 |
| Vomiting | 8.3 | 10.7 | 12.2 | 1.7 |
| Decreased appetite | 9.4 | 11.5 | 8.6 | 3.3 |
| Headache | 6.5 | 6.8 | 6.5 | 6.5 |
| Abdominal pain | 4.9 | 5.3 | 4.9 | 3.3 |
| Alopecia | 5.1 | 4.9 | 5.7 | 0.9 |
| Dizziness | 4.1 | 5.5 | 4.1 | 2.3 |
| Eructation (burping) | 3.8 | 5.2 | 5.6 | 0.6 |
| Injection-site reaction | 2.9 | 5.7 | 4.6 | 0.3 |
| Hepatic events | 0.3 | 0.3 | 0 | 0 |
| Cancer | 1.4 | 0.5 | 0.8 | 1.1 |
| Pancreatitis | 0.2 | 0.2 | 0.2 | 0.2 |
| Major adverse cardiovascular events | 0.6 | 0.8 | 0 | 0.8 |
| Cardiac disorders | 0 | 0.2 | 0.3 | 0.2 |
| Severe or serious gastrointestinal events | 1.7 | 3.1 | 3.3 | 1.1 |
| Gallbladder disease | 0.8 | 1.7 | 1 | 0.8 |
| Renal events | 0.3 | 0.3 | 0.3 | 0.2 |
| Major depressive disorder or suicidal ideation | 0.2 | 0.3 | 0.3 | 0 |
| Hypersensitivity | 0 | 0.2 | 0.2 | 0 |
| Hypoglycaemia | 1.4 | 1.6 | 1.6 | 0.2 |
| Cholelithiasis (gallstones) | 1.1 | 1.4 | 0.6 | 0.9 |
| Cholecystitis (gallbladder inflammation) | 0.6 | 0.5 | 0 | 0 |
SURMOUNT was a global trial over 72 weeks and subjects’ ages typically ranged from 35-60y, so while it was multi-racial, a longer intervention period or older/younger subjects may have yielded different results. Source: Jastreboff et al (2022). (Ref)
You can see below that the side effects lead to discontinuation of the trial in a relatively small number of subjects.
| Formulation | Proportion of participants who discontinued due to side effects |
|---|---|
| Placebo | 2.60% |
| Tirzepatide 5 mg | 4.30% |
| Tirzepatide 10 mg | 7.10% |
| Tirzepatide 15 mg | 6.20% |
Mortality
The first thing to say, is that higher doses were associated with a lower death rate, though these are small numbers across the board.
Gastrointestinal adversities
Gastrointestinal symptoms were the most common side effect, especially in patients starting the drug or increasing the dose. Mitigation strategies successful with other GLP-1 RAs include moderating dose escalation, avoiding exacerbating foods, and smaller more frequent meals. In the SURPASS trials the highest doses of tirzepatide caused more symptoms than semaglutide but, for equivalent weight loss and/or glycaemic control, caused fewer side effects. (Ref)
One of the functions of GLP-1 RAs is to slow the rate of food transit through the stomach, which may cause rare but serious side effects, including gastroparesis (stomach paralysis) and intestinal obstruction. This is rare enough that it has not been definitively established. However, the rate of gastric emptying is certainly slowed, which increases the risk of reflux. It also poses potential risks of pulmonary aspiration during general anaesthesia, a risk which has lead to additional pre-anesthetic protocols for this group. (Ref)
Gall bladder issues
Both an increase in gall bladder inflammation and gall stones has been observed with GLP-1RAs. These issues have also been observed with bariatric surgery and, as occurrence is proportional to weight loss, so it is probably weight loss, rather than GLP-1 RAs, driving gall bladder dysfunction. (Ref)
Pancreatitis and pancreatic cancer
Acute pancreatitis, or pancreatic inflammation, is extremely painful and may be deadly in up to 5% of cases. Incidence increases linearly with waist circumference. It is most commonly caused by gall bladder disease but other modifiable causes include heavy drinking, high blood triglycerides (fat in the blood) and some drugs, including GLP-1 RAs (Ref)
Acute pancreatitis is linked to pancreatic cancer, with one study (n=188,499) finding a history of acute pancreatitis associated with a 1.1% risk of pancreatic cancer over 5 years, compared to 0.2% in people who had not had acute pancreatitis. (Ref)
A retrospective study over 1.5 million initiators of GLP-1 RAs for obesity, found acute pancreatitis risk was 0.6% higher in GLP-1 RA initiators compared to similar non-users. In this case, there was no difference in chronic pancreatitis or pancreatic cancer, though this was only a year out from starting treatment. (Ref)
Against the risk of higher acute pancreatitis however, lower long term risk due to reduced waist circumference (and lower alcohol consumption) must be weighed.
Eye issues
Is GLP-1 RA use in diabetics associated with an increased risk of diabetic retinopathy and/or other eye disease? It depends.
A retrospective cohort study in adults with T2DM found GLP-1 RAs were linked to 7% higher retinopathy incidence over two-year’s follow up.
However, GLP-1 RAs were associated with significant protective effects in people with pre-existing retinopathy at therapy initiation, not just against retinopathy progression but also for a number of other conditions as well - including blindness. (Ref)
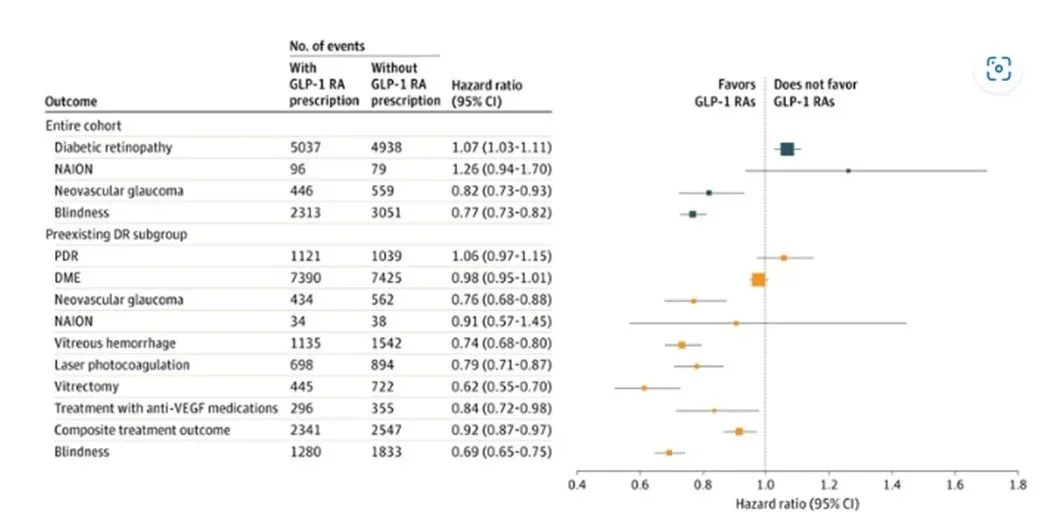
Outcomes from a cohort study assessing eye disease in diabetic patients on GLP-1 RAs compared to diabetic patients not on RAs (n = 370,132). Orang denotes the subgroup with preexisting diabetic retinopathy (DR) (n = 65,400) are shown in orange. Marker size is proportional to the mean total number of events in each category. DME: diabetic macular oedema; PDR: proliferative diabetic retinopathy; NAION: nonarteritic anterior ischemic optic neuropathy; VEGF: vascular endothelial growth factor. Source: Ramsey et al (2025). (Ref)
Alopecia
Semaglutide and tirzepatide are both associated with hair loss, particularly in women. This type of hair loss (technically, telogen effluvium) is not uncommon with dramatic weight loss, thus, it may again be the weight loss rather than the drug behind the issue. (Ref, Ref, Ref)
Low Mood
As noted, central to the effectiveness of GLP-1 RAs, is a reduction in dopamine-driven behaviour. While reducing unhelpful urges, it may also cause reduced motivation and low mood, a condition known as anhedonia. The tirzepatide trial included a modest signal for increased depressive disorders, while several other trials studying the interaction between GLP-1 RAs and mood have had mixed outcomes. Also relevant, any effect on mood has to be disentangled from nutrition-driven effects from reduced food intake, including lower leptin and higher cortisol, both also associated with depression. (Ref) This is an area of active investigation but for now the nature of the link, if any, is unclear.
The TGA conducted it’s own review, after reports of suicidal ideation by people taking GLP-1 RAs but did not find evidence of causality. It did however advise doctors to consider the benefits in patients with existing low mood - which, based on the prevalence of depression in the population, may constitute a substantial minority - and to monitor patients on therapy. (Ref)
Cost!!
Despite their effectiveness, 45% of people with diabetes and 65% with obesity discontinue GLP-1 therapy within a year, with lower income scaling directly with higher discontinuation rates. And, while most restart medication within two years, higher income predicts reinitiation, suggesting affordability is still a hurdle. Other factors for discontinuation cited in the same analysis include side-effects and having to inject yourself. The latter issue may be addressed if and when oral semaglutide is launched in Australia. (Ref) Other downsides, such as muscle loss or nutritional deficiencies, while real concerns, were not material factors in this analysis. (Ref, Ref) Also not mentioned was pregnancy, but this is also a reason for discontuing as data for use in pregnancy is not available. (Ref)
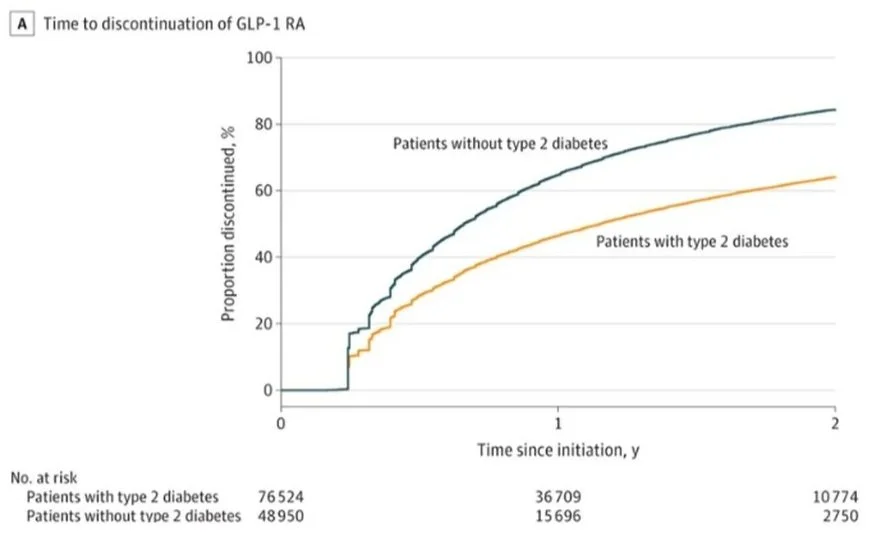
Discontinuation rates of GLP- 1 RAs. Source: Rodriguez et al (2025). (Ref)
This is US data. In Australia, Ozempic is subsidised for diabetes treatment, though not weight management, suggesting cost pressures will be greater in the latter group. With the advent of PBS reimbursement of Wegovy for weight management, in patients with symptomatic cardiovascular disease and a body mass index (BMI) ≥35 kg/m², or ≥32.5 kg/m² for people of Asian, Aboriginal, or Torres Strait Islander ethnicity, a small step toward improved affordability has been made.
In time, some of these medications will come off patent, at which point they will become cheaper. In the meantime, the case for PBS funding lies in demonstrating cost effectiveness. This is an involved process based on quantified cost benefit. If more clinical trials demonstrate better management of chronic disease, suggesting better health outcomes, then this may be possible, especially for discrete patient groups. (Ref)
What happens after you stop?
The World Health Organisation optimistically defines obesity as:
“a chronic, relapsing disease arising from complex interactions between genetics, neurobiology, eating behaviours, access to healthy diet, market forces, and the broader environment. “
On cessation of medication, neurobiology is quickly restored and the WHO’s other contributing factors typically remain as before. Hence, weight is generally rapidly regained along the same trajectory as weight loss through non pharmaceutical means. An extension of the STEP I trial (semaglutide) found a year after stopping treatment, participants regained two-thirds of lost weight, with cardiometabolic health deteriorating in line with weight regain. (Ref) The same results were found in SURMOUNT for tirzepatide. (Ref)
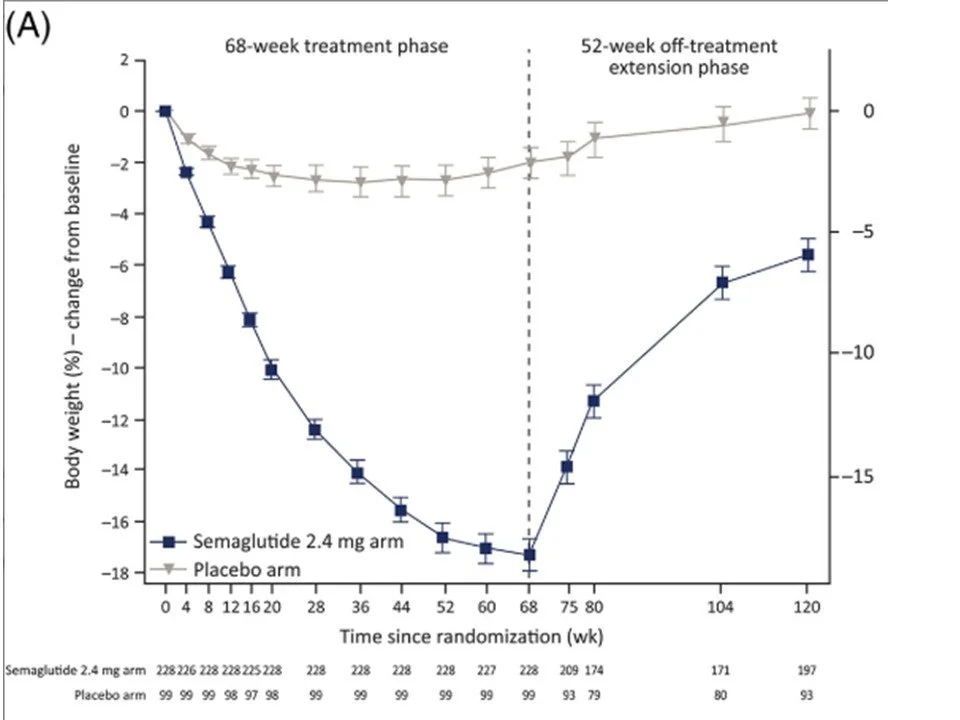
The STEP 1 trial extension: Weight regain after cessation of semaglutide. Wilding et al (2022). (Ref)
This points to a need for ongoing treatment as occurs with blood pressure, diabetes or cholesterol management. As GLP-1 RA weight loss might reduce or eliminate the need for these other medications and come with corollary metabolic benefits as we’ve discussed, this doesn’t sound like a bad trade off. Provided you are able to pay for it. However, as excess weight tends to increase in the population with deterioration in socioeconomic circumstances, in many cases, this will not be the case. There is some work ongoing with dose tapering and comprehensive dietary interventions which shows promise, but again, this may not be available to those who most need it. (Ref)
Perhaps the greater benefit will be in an improvement in the food environment, as profitability from constant extortions nudges to consume hyper-palatable foods reduce. Consumer data already shows people taking GLP-1 RAs disproportionately reduce food purchases of processed foods and sugar-sweetened beverages. (Ref) Perhaps Coca-Cola and McDonald’s won’t be able to justify the expense of being major FIFA World Cup sponsors in the future and David Beckham won’t have to support his needy family by hawking Mc Donald’s in the Better World of the future. (Ref)

FIFA’s Official 2026 Partners include several food and beverage companies which contributed 40% of sponsorship funds. Besides Coca-Cola and McDonald’s, Budweiser (Anheuser-Busch), Frito-Lay (Lay’s), Mengniu Dairy, Unilever, and Diageo also feature. (Ref)
Conclusion
So what do you think? Panacea? Burdensome life-long commitment? Both? Cards on the table, while they won’t work for everybody, I think they’re a boon. Practitioners and patients finally have something that will move the needle on intractable conditions like diabetes and weight, conditions responsible for so much ill health and many deaths in our population. Cardiovascular and (possible) cancer benefits, along with a potential role in addiction management are also something we all should welcome as these impact us all.
Lifelong injections are hard to accept, especially if your underlying reason for initiating it has resolved. Moreover, the cost is impossible to ignore. Longer term though, therapy will become more nuanced and a change in the food environment may now be possible. Not this time via government policy, as occurred with smoking and how we all thought it would happen. Eventually. But instead via a bottom reduction in demand from individuals.
I am very aware that nutrition during weight loss, when food intake is much reduced, and holding onto losses if you stop therapy are both topics that deserve particular attention and where data is fast emerging. We’ll cover them in future articles.