
Strong Bones for Life: Part 1

Ah dear, you’d think I would have learnt by now. What was going to be one article will now be four. This article will look at the bigger osteoporosis picture and some lesser known lifestyle and nutrition factors. The following three articles will look at three protective nutrients: calcium, vitamin D and vitamin K. Much of the research is in women but, as bone weakness is not a trivial issue in men, I’ve tried to include them where I could. Let’s begin!
Osteoporosis? osteopenia? What’s the difference?
Osteopenia and osteoporosis occur on a continuum and represent reduced bone mineral density. From here, we’ll group them together and call them bone weakness.
In Australia, bone weakness is diagnosed by measuring bone mineral density (BMD) using dual-energy x-ray absorptiometry (DEXA). Young healthy adults of the same sex as you form your reference group and are assigned a T-score of 0, so a T-score below 0 represents lower bone density than these young adults. As bone is lost from about the age of 25 onwards, this would be the case for most people who are no longer 25. It is only when the T-score reaches -1 that a diagnosis of osteopenia is made, while a T-score of -2.5 or less is diagnostic for osteoporosis.
T-score cut-offs
Normal: 1 to -1
Osteopenia: -1 to -2.5
Osteoporosis: -2.5 or less
Here’s what a DEXA report might look like:
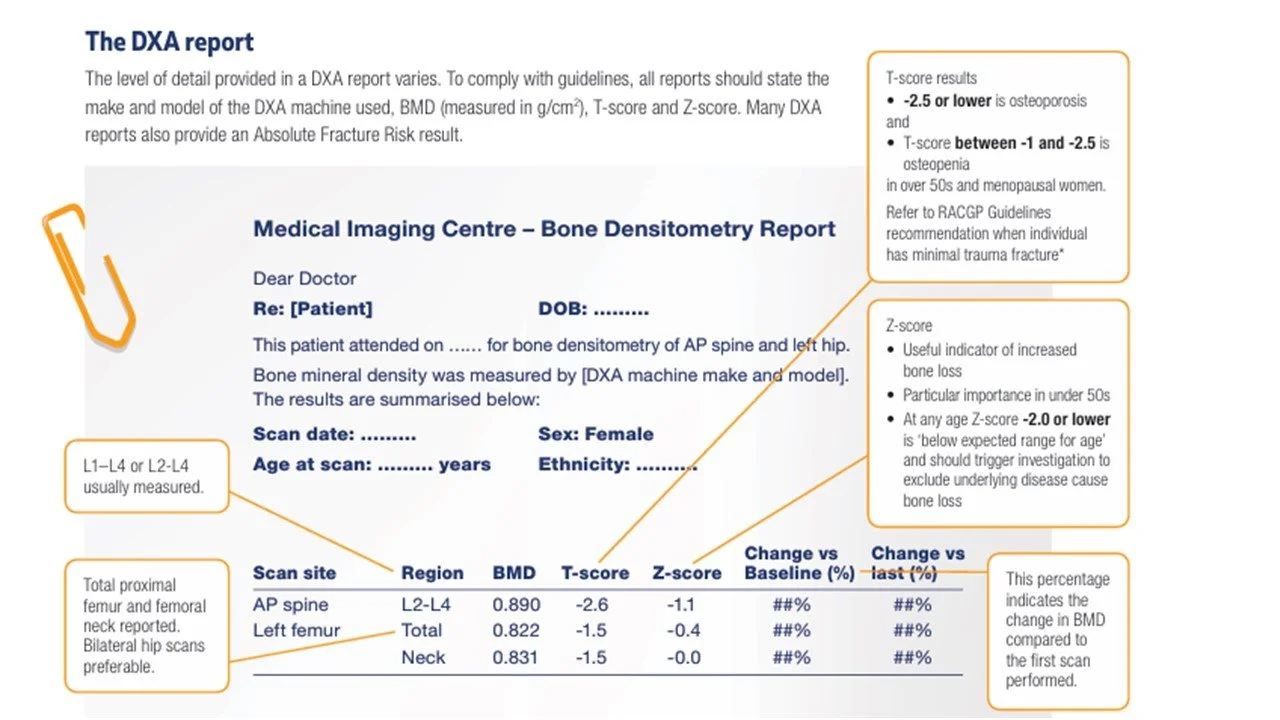
Source: Healthy Bones Australia (2025). (Ref) L1-L4 or L2-L4: lumbar vertebrae L1/L2-L4; neck refers to the femoral neck, which is the hip.
Armed with a DEXA, you can check your bone health using this Australian online assessment tool:
Know Your Bones - Self Assess Your Bone Health Now!
Yes, yes, my bones are ageing like the rest of me but what does this mean for my future prospects?
Both osteoporosis and osteopenia increase fracture risk and in 2023, about 190 thousand people suffered a minimal trauma fracture – the type of fracture that usually occurs with bone weakness. Some two thirds of these people were hospitalised, the majority with a hip fracture: the most problematic type. (Ref) A Victorian study revealed that in people who had a first hip fracture, the majority were women, and nearly half were at least 85. Eight percent of patients died within 30 days of the fracture and 25% within a year. (Ref)
Perhaps, less discussed however are non-fatal fractures which fail to heal perfectly, resulting in chronic pain, muscle wasting, disability, loss of independence and premature death. Or even with good recovery, a fear of subsequent fracture which curtails physical activity and so further undermines bone and muscle strength. (Ref) It’s worth considering also that more than half of women who sustain a fragility fracture are merely osteopenic and have not yet progressed to osteoporosis. (Ref)
Finally, while it doesn’t directly affect your future prospects, it costs a lot. The cost of bone weakness in Australia in 2023 was an estimated $4.8 billion. (Ref)
Who’s affected
Coming as a surprise to no one, women, specifically older women have the weakest bones and thus are most at risk. However, you might not be aware how common bone weakness is; that bone weakness is already apparent in many people in their fifties; and that it’s common in both sexes.
In 2023, based on data from the Geelong Osteoporosis Study, an estimated 67% of Australians over 50 had bone weakness and about a quarter of these people had osteoporosis. (Ref, Ref) Using the Geelong study, the chart below depicts the prevalence of bone weakness in women and men over 50 in pink and blue, respectively, while the yellow line shows the proportion of people predicted to have a fracture in that year in each group.
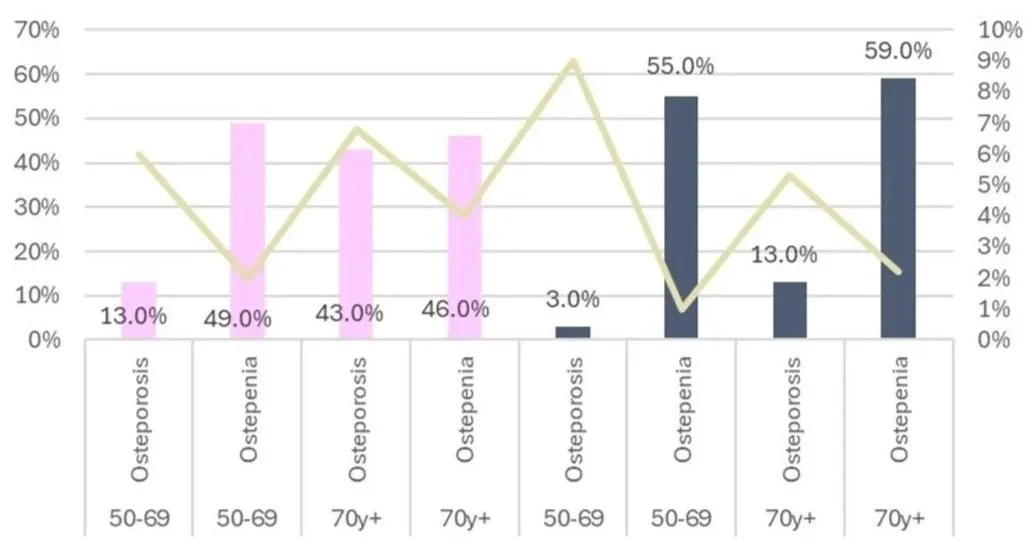
The prevalence of bone weakness in women (pink) and men (blue) [plotted on the left axis], while the yellow line shows the proportion of people predicted to have a fracture in that year in each group [plotted on the right axis].
Data source: Healthy Bones Australia (2024). (Ref)
If you are an older woman, you are very likely to be referred for a DEXA scan at some point. However, DEXA is not generally rebated by Medicare unless you are a woman over 70, so if you’re a younger woman or a man, though you may also have low bone density, you may not find this out until you break a bone, and possibly not even then. In fact, self-reported rates of osteopenia and osteoporosis are much lower than the findings of the Geelong study, suggesting many Australians have poor bone health but just don’t know it. (Ref)
Lacking a DEXA scan for reference, loss of height can be a useful indicator you can measure yourself, and here’s why: vertebral fractures are the most common osteoporotic fractures before age 75, accounting for 48% of fractures in men and 39% in women over 50. But they usually remain unrecognised, and thus an opportunity to guard against further osteoporotic fracture risk is lost. Data from the European Prospective Osteoporosis Study found each centimetre of height lost increased the risk of pre-existing vertebral fracture by 6%. (Ref)

A lumbar fracture caused by bone weakness
Source: He et al (2021). (Ref)
Yikes. What can I do?
You’re stuck with your sex, age and genes. And there are other factors, such as medical conditions and some medications that can compromise bone strength, listed in the figure below, but we won’t cover all those here. Instead we’ll look at the dietary and lifestyle levers at your disposal.
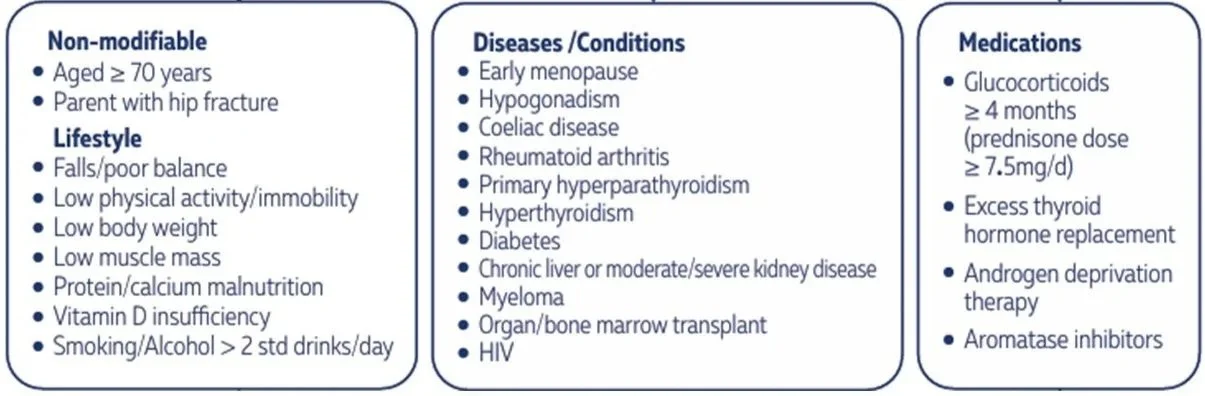
Risk factors for weak bones.
Source: Healthy Bones Australia (2024). (Ref)
1. Start Early (possibly not something available to you but for the young people in your life)
Childhood sets the scene for bone health throughout life as weaker bones in childhood tend to stay weaker into adulthood. In pre-adolescent childhood, fractures (especially in children lacking derring-do) should raise a question mark, as imaging shows these children often have weaker bones than their peers. Fortunately, during childhood and adolescence (especially at the onset of puberty) the growing bone is particularly responsive to the same exercise and nutrition interventions outlined in this and the following three articles. (Ref)
The aim of the game is to maximise bone mineral density during growth to establish a greater reserve to draw upon over the rest of life (and a greater reserve from adolescence onwards is one reason men’s bones stay stronger for longer than women’s). By late adolescence, the body is less responsive to efforts to increase bone density but the body continues to lay down mineral into adulthood, with peak bone mass (PBM) not reached until the mid-twenties. The study below of a population of Caucasian young people, found PBM was reached at 22y in women and 27y in men. (Ref)
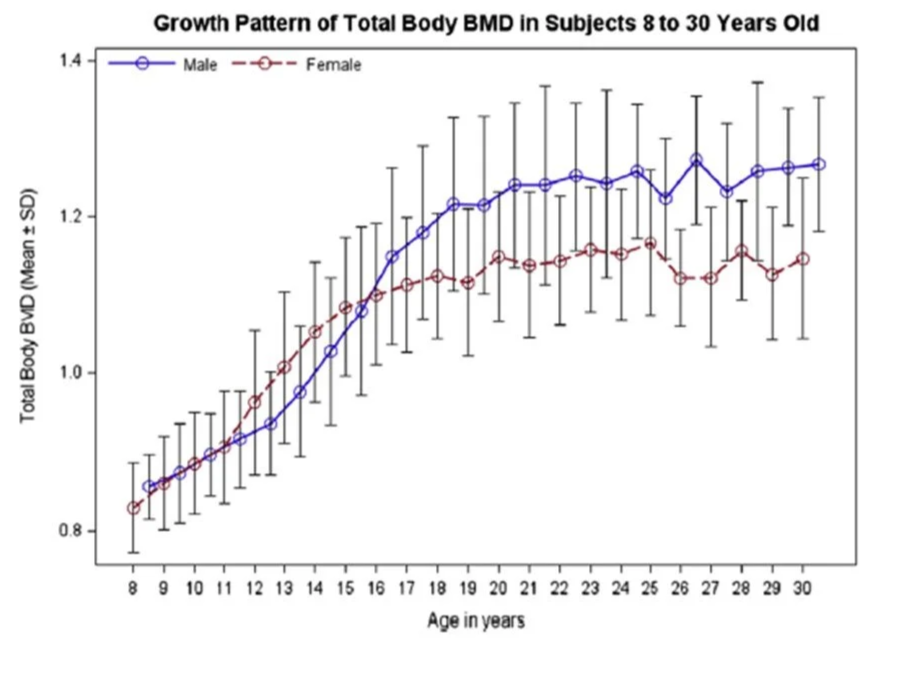
Source: Lu et al (2016). (Ref)
2. Exercise – harder is much better
The LIFTMOR study was an eight month trial comparing high intensity exercise (HiRIT: a combination of heavy load weight training and high impact exercise) to low intensity exercise (CON: designed to improve balance and mobility) in 101 postmenopausal women (average age 65y) with bone weakness. The results were pronounced, with the HiRIT group gaining bone mass (they even grew a little taller), while the CON group lost bone mass. The HiRIT group also gained strength and their gains in flexibility, an area targeted by the CON program, were also greater in the HiRIT group. (Ref) These lessons do not just apply to women, as bone gains in men have been demonstrated in other trials. (Ref) Check out LIFTMORE’s results.
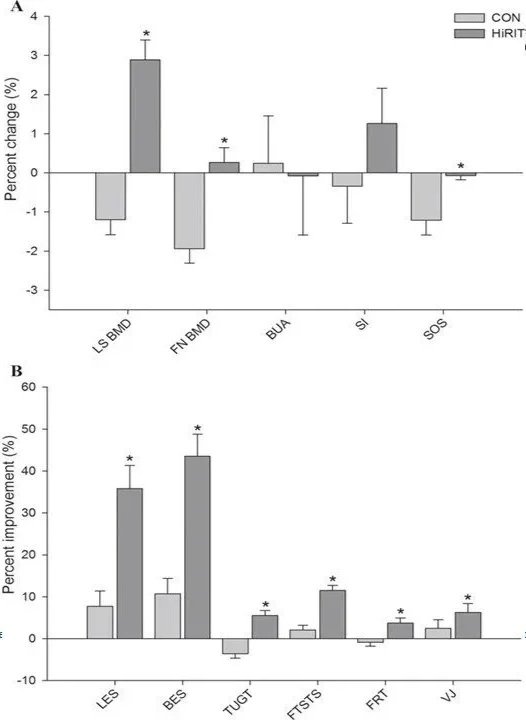
Change in (A) bone and (B) physical performance for HiRIT and CON after an 8-month exercise intervention in postmenopausal women with low bone mass (n = 101). LS = lumbar spine; BMD = bone mineral density; FN = femoral neck; BUA = broadband ultrasound attenuation; SI = stiffness index; SOS = speed of sound; LES = leg extensor strength; BES = back extensor strength; TUGT = timed up-and-go test; FTSTS = five times sit-to-stand; FRT = functional reach test; VJ = vertical jump. *Indicates between-group difference (p < 0.05).
Data source: Watson et al (2017). (Ref)
You might be wondering about injury or thinking this is all sounds rather hard, two familiar hurdles to exercise consistency, but LIFTMORE’s results suggest these weren’t big issues in practice. LIFTMORE’s HiRIT subjects exercised in groups of eight with an instructor, while CON was an at-home program. Neither program can have been too unpleasant as both programs saw good adherence being 92% for HiRIT and 85% for CON and there was a single short term muscle strain injury in the HiRIT group over the eight months. (Ref) So small group classes seem like the way to go. Also, while it’s no substitute for one-on-one instruction, Healthy Bones Australia, has published a report (here) targeted at physiotherapists and exercise physiologists, but nevertheless an excellent resource for anyone who wants evidence backed guidance.
3. Smoking
The effects of smoking on bone density have been known for decades, with more smoking linked to greater bone weakness. And the relationship survives adjustment for smokers being lighter, younger at menopause and exercising less, to suggest an independent effect of smoking on bone. In particular, smoking can increase lifetime hip fracture risk by 31% in women and 40% in men. Fortunately, the risks can be partially reversed by giving it up. (Ref) As to vapes, they appear less harmful than cigarettes but population studies suggest vapers have higher rates of fracture, even when adjusted for other factors, than never vapers. (Ref, Ref)
4. Alcohol
Likewise, even quite low levels of alcohol are associated with bone weakness. A 2019 review found one to two drinks per day increased the risk of osteoporosis by 1.34 times, while more than two drinks had 1.63 times the risk. (Ref) Of course, falls and thus fractures are also more likely after a few drinks.
5. Estrogens
Several pharmaceuticals are effective agents in mitigating bone weakness (generally osteoporosis). Amongst these, hormone replacement therapy (HRT, now known as menopausal hormonal therapy (MHT)) is indicated for bone weakness in many post-menopausal women <65y, without a history of breast cancer. (Ref)
If MHT/HRT is out for you, or even if it’s not, then the phytoestrogen genistein is well worth considering. Soy foods are by far the best source of genistein, typically containing 81mg/100g of soybeans (which is an adequate dose for our purposes). (Ref) In an Italian twelve-month randomised controlled trial in 90 women, aged 47 – 57 years, genistein increased bone density in the femoral neck and the lumbar spine as effectively as HRT, while bone was lost in the placebo group. The results are shown below. (Ref)
Providing further support, a meta-analysis of 63 randomised controlled trials in postmenopausal women, found genistein significantly increased BMD compared to placebo in the spine, hip and wrist and that 54mg/day of of genistein appeared to be the sweet spot for results. (Ref)
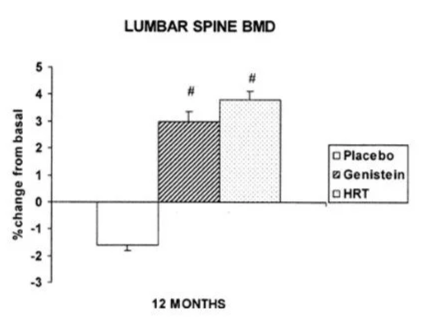
Data source: Marbito et al (2002). (Ref)
And no. Soy is not associated with increased breast cancer risk. In fact, soy appears protective both in women who have never had breast cancer, as well as against recurrence in those who have. (Ref, Ref) Also: Soy also may have protective affects against prostate cancer risk (Ref); infants fed soy did not experience onset of puberty at an earlier or later point than those that were not (Ref); and nor does soy lower male hormone levels or have feminising effects in men. (Ref) Soy needs better PR!
6. Body weight
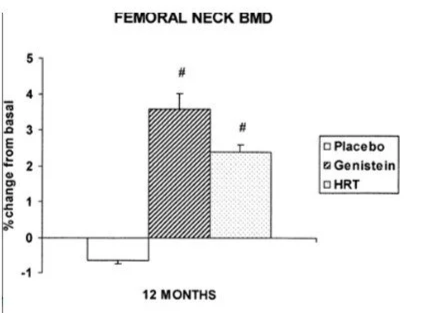
Bone health is one area where higher body weight can be protective. The Women’s Health Initiative (WHI) examined the relationship between body composition and bone health in 78,000 Caucasian post-menopausal women, finding bone density increased with lean body mass (often used interchangeably with muscle mass). Even though bone density didn’t quite increase one to one with total weight, nevertheless, fracture risk, at least in that riskiest of areas, the hip, as well as the trunk, fell considerably as weight increased. (Ref)
Relative fracture incidence in cases per 1000 person-years by body mass index category after adjustment for age, hormone use, and diabetes. *p < 0.05 vs. healthy weight.
Source: Beck et al (2009). (Ref)
6. Anti-inflammatory Diet
Inflammation is one of those catch-all terms in health that’s often rather ill-defined and which may seem more about marketing than anything else. But, at least in nutrition, an attempt has been made to add some scientific objectivity with the dietary inflammatory index (DII).
The DII is a validated methodology that quantifies the inflammatory effects of foods based on biochemical markers. (Ref) You’ll want to know what an anti-inflammatory diet looks like and it tends to be heavy on fruits, vegetables, legumes nuts, seeds, spices and seafood and lower in land-based animal products (particularly those high in iron and/or saturated fat) and processed foods. (Ref)
A British longitudinal study over eight years in 1577 men and 2071 women and adjusted for 10 potential confounders found the 20% of women with the most inflammatory diets had a 46% higher chance of fracture compared to the 20% with the least inflammatory diets. However, the relationship in men was not statistically significant. (Ref) Turning to US NHANES data, the third of people with the most inflammatory diets had a 73% greater risk of osteoporosis than the third with the least inflammatory diets after adjustment for a range of factors. But again, although there was a trend, these results were only statistically significant in women. (Ref)
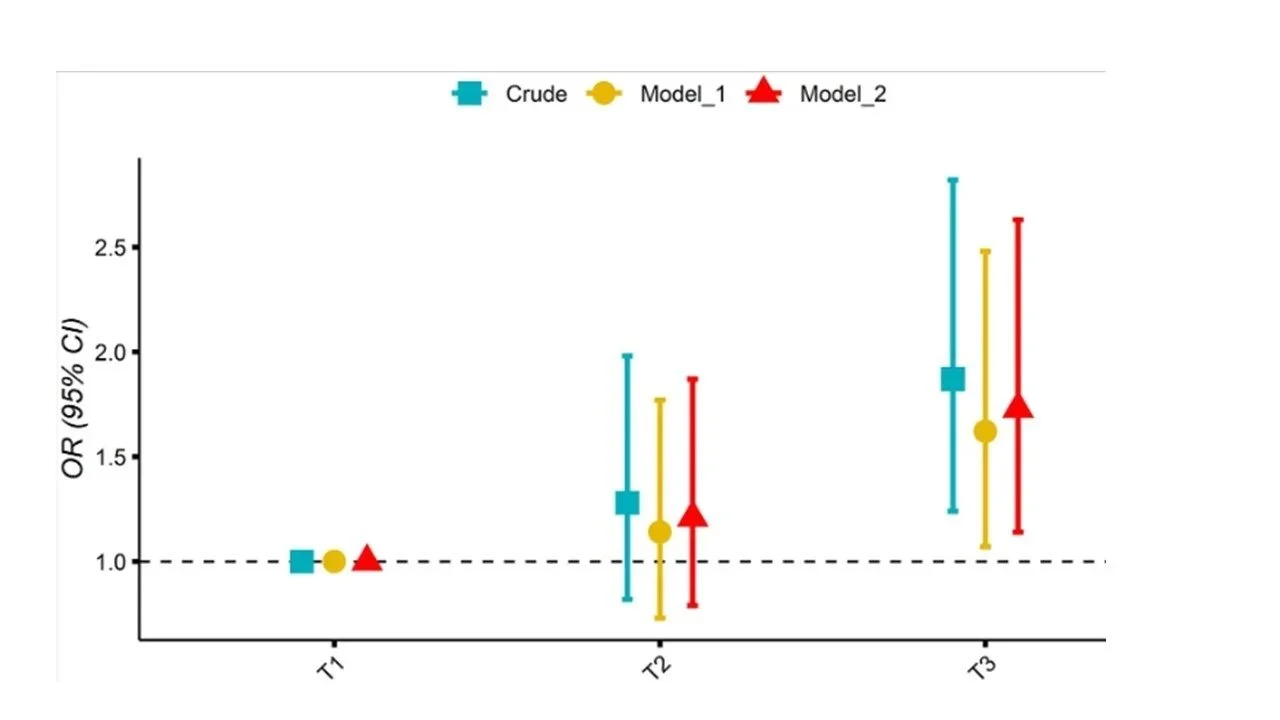
Association of the DII with with osteoporosis. T1 is the third of subjects eating the least inflammatory diet based on the DII, T2 is the middle third, and T3 subjects ate the most inflammatory diet. Model 1 is adjusted for age and sex; while model 2 is adjusted for age, sex, hypertension, smoking status, physical activity, history of fracture, diabetes, race, BMI, education, history of prednisone or cortisone, calcium intake, alcohol use, and poverty index.
Source: Chen et al (2022). (Ref)
7. And two things that don’t appear to make a difference but that you may have heard do
Coffee and tea
Good news! Although, there has been suggestion that coffee and tea may increase osteoporosis risk, the converse is true. A 2025 meta-analysis of 14 observational studies comprising half a million people, found coffee consumption was linked to a 21% reduction in risk, while tea was associated with 25% reduction. Amongst coffee drinkers, more than one cup a day was more protective than less than one cup a day, while for tea, more than four cups a tea per week was more protective that less frequent intake. (Ref) You may think this was a result of more milk consumption rather than the coffee and tea per se, but most studies, though not all, adjusted for calcium intake.
Salt
The Australian 2017 dietary guidelines tell us that increased salt consumption causes increased losses through the kidney and cautions salt moderation to reduce this effect. (Ref) Most of us would be better off eating less salt but, as far as calcium goes, this view has evolved. Yes, salt increases calcium loss in the kidney but it also improved absorption in the intestine and the net effect is insignificant. The Women’s Health Initiative (WHI), a gift that keeps on giving, found no association in adjusted models between salt intake and bone weakness or fracture at any site over six years’ observation. (Ref)
Conclusion
That’s it for now. There’s quite a lot to say on calcium, vitamin D and vitamin K, which are all important for bone health and all have other functions too. One final word, like many health conditions, for optimal bone outcomes, treat each factor as a member of an orchestra, important but reliant on the other players for optimal results.