
Vitamin K. Special K

Vitamin K is possibly the least discussed vitamin. It sits off to the side, absent from nutrition panels and with a weird name, so no one ever thinks much about it unless they have a blood clot or rat bait poisoning. But behind the scenes, research has been finding vitamin K is valuable beyond blood clotting, with varying degrees of evidence supporting protective effects against four of the health scourges of our times: cardiovascular disease, dementia, diabetes and osteoporosis. It’s not all that easy to get protective doses from food, though possible! Failing that supplementation is cheap and safe and I think will become a mainstay of treatment protocols for chronic disease.
This is the fourth article on our bone health series.
| Full name | Abbreviated name | What it is |
|---|---|---|
| Phylloquinone | Vitamin K1 | |
| Menaquinone | Vitamin K2 | |
| Menaquinone-4 | MK-4 | A common K2 vitamer |
| Menaquinone-7 | MK-7 | An important K2 vitamer |
| (Un)carboxylated osteocalcin | (u)cOC | The degree of carboxylation is a measure of vitamin K adequacy |
| (Un)carboxylated matrix Gla protein | (u)cMGP | As above |
Vitamin K is so called as it is vital for blood koagulation (this was a Danish discovery). Like several vitamins, vitamin K is not a single entity but refers to a group of structurally similar variants, chief of which are phylloquinone (K1) and menaquinone (K2). Parsing further, there are ten K2 vitamers range from MK-4 to MK-13, of which menaquinone-4 (MK-4) and menaquinone-7 (MK-7) are the most significant and well studied. (Ref)
Sources
Vitamin K1 is the main form of vitamin K in the diet. It’s made by plants and found in leafy green vegetables.
Vitamin K2 is produced by bacterial fermentation, with different bacteria producing different K2 vitamers.
MK-4 is found in animal produce where it’s mainly a product of absorption of K2 produced by the gut bacteria (remembering that most food animals are ruminants or semi-ruminants so the gut microbiota is not restricted to the colon as it is in humans. (Ref)
MK-7 and other K2 vitamers are found in fermented foods such as cheese and, in heroic amounts, in the Japanese fermented food natto, which is an impressively rich source of MK-7. (Ref)
Vitamin K2 supplements are generally MK-7 and the same bacteria used to make natto, Bacillus subtilis, is generally used for supplement manufacture due to its safety and ease of use. (Ref)
In Japan, MK-7 intake is relatively high due to the consumption of natto (natto consumers averaging 154 μg/d) (Ref)
MK-7 to MK-10 consumption is more common in cheese enthusiast populations, such as those of Northern Europe, where lactic acid bacteria (mainly MK-8 and MK-9) and propionic acid bacteria (mainly MK-10) are commonly used in cheese production. (Ref, Ref) One Dutch survey found MK-5 to MK-10 intakes were 22 μg/d. Thus, much less than Japanese Natto eaters. (Ref)
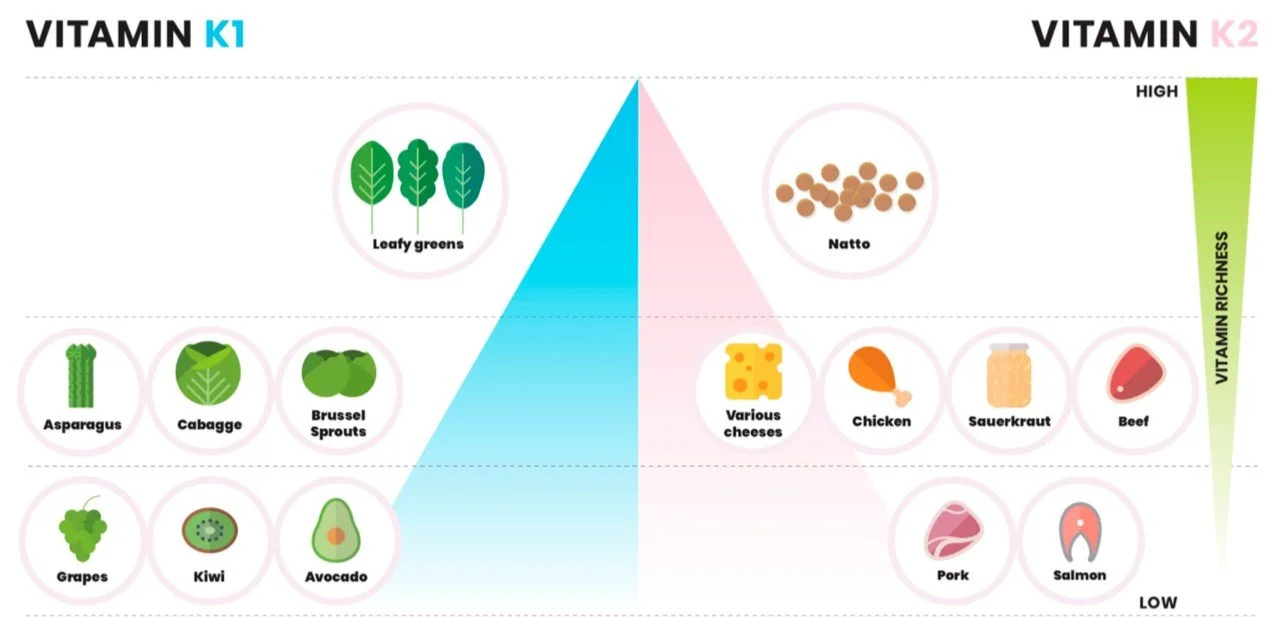
Dietary sources of vitamin K. Source: Halder et al (2019). (Ref)
The table below shows vitamin K content detected in samples of Australian foods from one study. (Ref) Note though, that vitamin K content is highly variable based on crop, location, time since harvest, fermentation method and duration etc. Moreover, though cooking does not greatly alter vitamin K1 content, natural and artificial light quite dramatically do. (Ref) All this makes food-based assessments fairly poor to assess intake with any rigor.
| µg / 100g | K1 | MK-4 | MK-7 |
|---|---|---|---|
| Spinach | 263 | ||
| Kale | 129 | ||
| Cabbage | 70 | ||
| Broccoli | 68 | ||
| Lettuce | 26 | ||
| Canola oil | 75 | ||
| Margarine | 69 | ||
| Olive oil | 44 | ||
| Butter | 25 | ||
| Egg | 33 | ||
| Chicken | 26 | ||
| Beef | 16 | ||
| Thickened cream | 20 | ||
| Natto* | 82 |
*this is about 90% lower than every other other reference I found.
How much do we need?
The Australian Dietary Guidelines publish Adequate Intakes (AIs), which lack the scientific exactitude of recommended dietary intakes. Instead, AIs are based on the highest median intakes in an age group and gender, with the reasoning that they’re adequate for normal blood clotting and also enough to sustain seeming general health. (Ref)
Vitamin K adequate intakes (Ref)
| Age | Male | Female | Pregnancy | Lactation |
|---|---|---|---|---|
| Birth to 6 months* | 2.0 µg | 2.0 µg | ||
| 7–12 months | 2.5 µg | 2.5 µg | ||
| 1–3 years | 30 µg | 30 µg | ||
| 4–8 years | 35 µg | 35 µg | ||
| 9–13 years | 45 µg | 45 µg | ||
| 14–18 years | 55 µg | 55 µg | 60 µg | 60 µg |
| 19+ years | 70 µg | 60 µg | 60 µg | 60 µg |
*assumes infants receive prophylactic vitamin K at birth.
These values are based on survey data, which is now over 30 years old and, in any case, as already outlined, vitamin K is not consistent in food across time and regions. Nor would this measurement breakdown vitamin K intake into K1 or K2, let alone into K2 variants. (Ref)
Also, these AIs are set purely with a view to adequate blood clotting. By this measure, virtually no one is vitamin K deficient as vitamin K-dependent coagulation factors are fully carboxylated (that is, activated) in normal adults. However, other vitamin K-dependent proteins are not. For instance, about a quarter both of osteocalcin and matrix Gla were found to be uncarboxylated (and thus inactive) in apparently healthy adults in one study, which, as we will see, has consequences for bone and cardiovascular health. (Ref)
Physiology
K1 comes tightly bound to plant chloroplasts so is not generally well absorbed. (Ref) Cooking doesn’t improve K1 absorption, however co-ingestion of fat does up to three-fold. The largest source of vitamin K in the diet is lettuce and therefore the AI takes account of this poor absorption. K2 however is unbound and therefore generally well absorbed as long as fat is also present.
Post absorption, K1 briefly circulates in the blood but within 24h is sequestered in the liver from whence it exerts its actions. K2 is more active outside the liver. MK-4 is also rapidly removed, however, MK-9 persists for 2-3 days and MK-7 for up to four days in the blood post ingestion. (Ref) You can see blood serum tenure of K1 an MK-7 compared below.
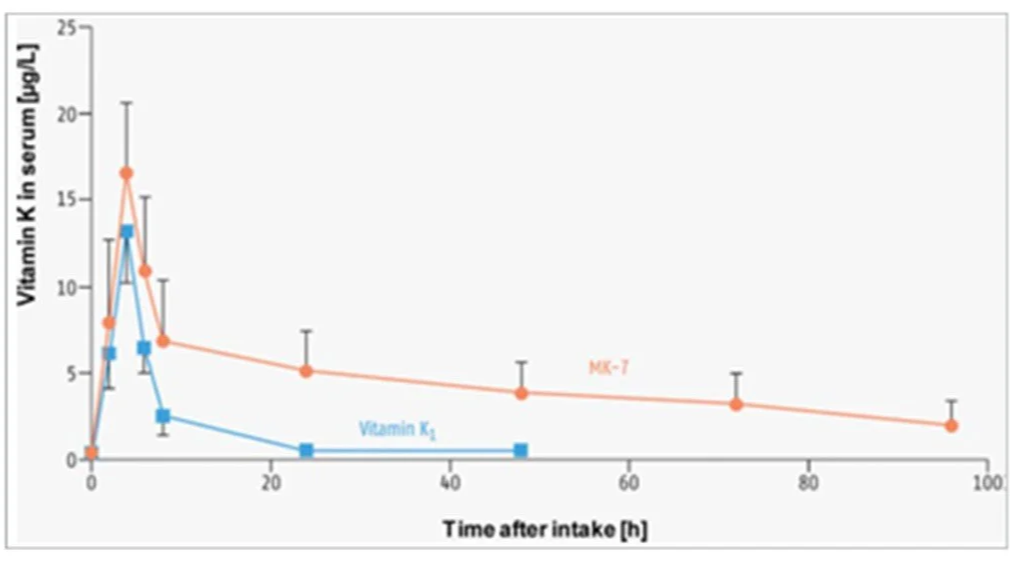
Persistence of MK-7 in blood serum compared to K1. Source: Gröber et al (2014). (Ref)
As in fermented food, bacteria in the human gut also produce K2, and there is a little evidence that this may be at least partially absorbed.
Nineteen vitamin K-dependent proteins have been identified, where vitamin K is a cofactor for enzyme activation of these proteins via carboxylation. (Ref, Ref) The actions of all of these proteins have not been fully elucidated (and there may be more proteins yet discoverable), thus the scope of our knowledge of vitamin K’s actions is incomplete. For now, Vitamin K’s best known functions are in blood clotting, a role generally ascribed to K1 and occurring in the liver, while vitamin K2, particularly MK-7 promotes bone strength and cardiovascular health, with the latter extending to cognitive health. (Ref) Matrix Gla protein (MGP) and Osteocalcin are two important vitamin K-dependent proteins.
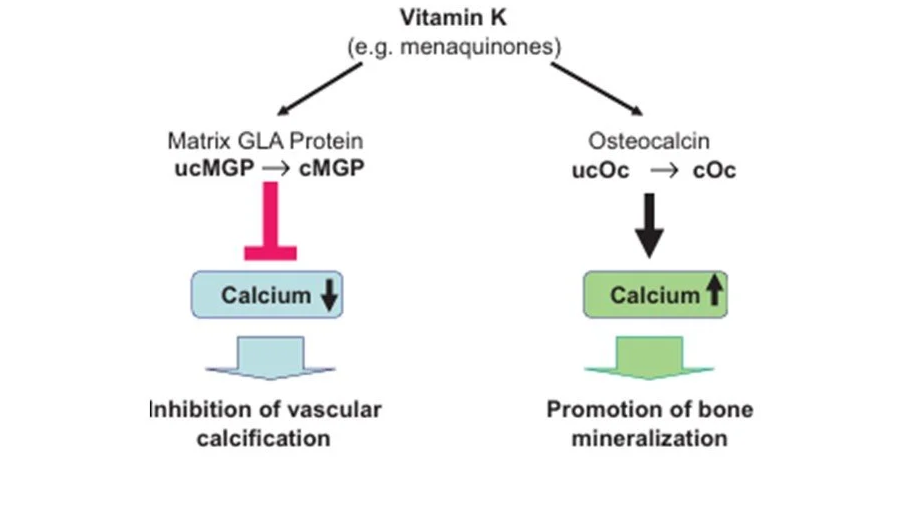
Functions of vitamin K2. Source: Gröber et al (2014). (Ref) ucMGP = uncarboxylated matrix Gla protein; cMGP = carboxylated matrix Gla protein; ucOC = uncarboxylated osteocalcin; cOC = carboxylated osteocalcin
Prove it – studies please
Glad you asked.
Bone Health
Osteocalcin is made by osteoblasts (bone forming cells) in the bone. Osteocalcin (OC) is activated through a reaction with vitamin K to become carboxylated (cOC). Once activated, it attracts and binds calcium thereby enhancing bone strength. There is also some evidence that osteocalcin may play a role in enhancing insulin sensitivity and glucose tolerance. (Ref)
As the chart below shows, vitamin K1 can activate osteocalcin but, as it is rapidly removed from circulation, not very effectively. Nevertheless, unless you’re Japanese, it’s probably doing the heavy lifting in this regard. Due to it’s persistence in the circulation, MK-7 tends to accumulate with daily dosing and thus is much more effective for osteocalcin activation. High levels of uncarboxylated osteocalcin (ucOC) are a marker of vitamin K deficiency and a risk factor for fractures.
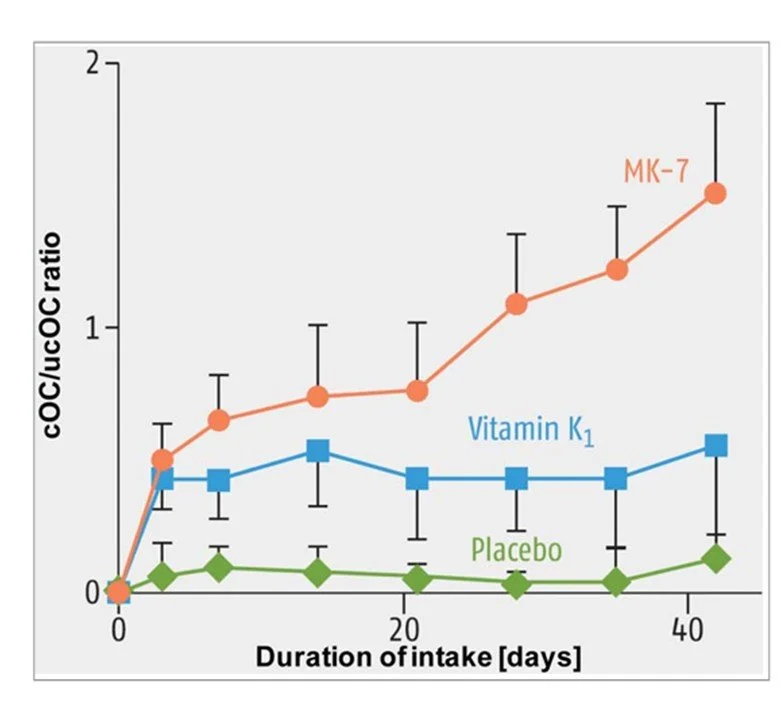
The relative ability of K1 and MK-7 to carboxylate osteocalcin. Source: Gröber et al (2014). (Ref)
In a 3-year trial in 244 postmenopausal women, 180 μg MK-7/day significantly improved vitamin K status and reduced the age-related decline bone mineral density (BMD) in the lumbar spine and femoral neck. (Ref)
In the Nurses’ Health Study (n = 72,327, average age 63y), over 10 years, the rate of hip fracture in women with vitamin K intake >109 mg/d was 30% less than in women with intakes <109 mg/d (RR: 0.70; 95% CI: 0.53, 0.93). Here, women who ate lettuce (ie K1) daily had a 45% lower risk of hip fracture rate than women who consumed lettuce no more than once weekly. (Ref)
A 2022 meta-analysis (9 RCTs, n = 6853 subjects) found K2 was associated with enhanced lumbar and forearm BMD. (Ref)
A 2021 meta-analysis (10 RCTs, 1,346 subjects) found vitamin K combined with calcium was associated with improved lumbar BMD compared to control. Vitamin K2 was more efficacious than K1. (Ref)
Finally the following chart isn’t great science but but it’s interesting to see how natto consumption in Japan by region is inversely correlated with hip fracture risk, especially as vitamin D would likely be lower in the North. (Ref)
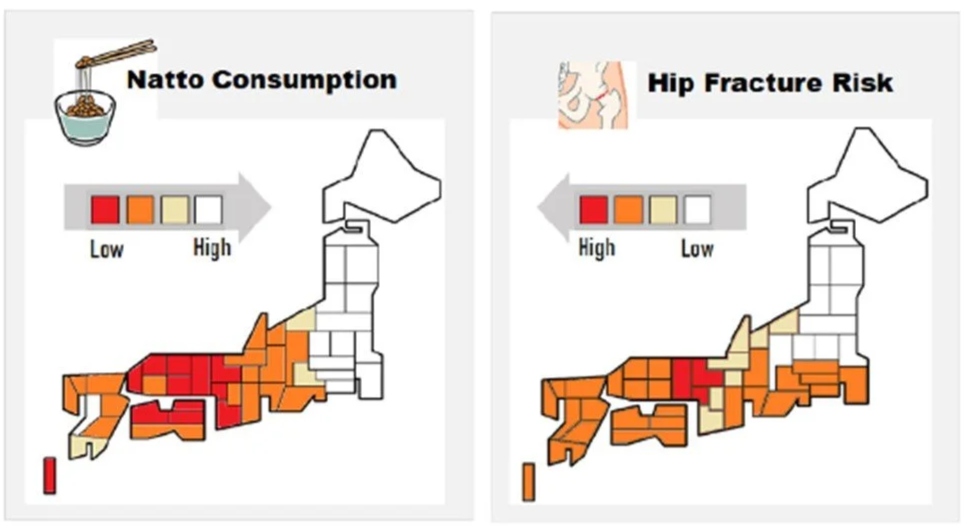
Source: Sato et al (2020). (Ref)
Cardiovascular Health
Another vitamin K-dependent protein is matrix Gla protein (MGP), which is synthesized in the arterial walls. Warfarin is garden variety rat bait but also still used sometimes in people at risk of blood clots as it blocks the action of vitamin K. Genetic mutations which block MGP activation and/or long term warfarin use, are both associated with arterial calcification providing mechanistic evidence for the importance of vitamin K in cardiovascular disease. Moreover, as it is now accepted that cardiovascular disease is a major contributor to cognitive decline, vitamin K’s cardioprotective function likely extends to brain health.
The evidence is supportive though not overwhelming as yet. As with osteocalcin, high levels of uncarboxylated MGP (uMGP) are a marker of vitamin K deficiency and often used as a surrogate in observational studies. People on anti-coagulant therapy are also often studied as a proxy for low vitamin K status (as vitamin K action is reduced). Here K2, specifically MK-7 has the most evidence of benefit for arterial calcification. (Ref)
| AVADEC trial: N=304 male subjects | Double blind RCT | MK-7 (720 μg/d) + vitamin D (25 μg/d) or placebo for 2y | In subjects with high arterial calcification plaque at baseline, calcification was slower in the intervention group than placebo though there was no difference in non-calcified plaque volume. The number of cardiovascular adverse events was also lower in intervention subjects, regardless of calcification at baseline. |
Hasific et al (2023) (Ref)
| Study subjects | Design | IResults |
|---|---|---|
| Rotterdam study: N = 4,807, >55y. | Observational trial over 10y | In the middle and upper tertiles (>32.7 µg/d) of K2 intake, compared to the lowest K2 tertile (<21.6 µg/d): Risk of heart disease was 27% and 57% lower; all-cause mortality was 9% and 26% lower; and severe aortic calcification was 29% and 52% lower. K1 intake (>250 mg/d) was not related to any of the outcomes. All results were adjusted for other lifestyle factors. |
| EPIC study: n = 40,011 subjects. At baseline, 518 subjects had type 2 diabetes. | Observational trial over 11.2y | Lower levels of MGP carboxylation were associated with 21% higher risk of CVD, 32% higher peripheral artery disease, and 75% higher heart failure after adjustment. |
| A meta-analysis (6 RCTs, n = 77,643 subjects and 2 observational studies, n = 19,952 subjects) | Traditional long-term vitamin K antagonists (VKAs) eg warfarin, compared to novel anti-coagulants (NOACs) | NOACs were marginally protective against cognitive impairment compared to VKAs |
Geleijnse et al (2004) (Ref); Dalmeijer et al (2013) (Ref); Zhang et al (2019) (Ref)
Dose?
Research to date suggests doses of 45 μg/d and 90 μg/d of MK-7 are required to move the needle on cardiovascular health. (Ref) Meanwhile, an excellent review on the subject found 100 µg/d MK-7 was effective in all adults to improve osteocalcin activation over 4 to 12 weeks and thus represents a sensible lower bound to cover both heart and bone outcomes. (Ref) Providing some assurance on high intakes, the AVADEC trial subjects (who were elderly men) received 720 µg/d for two years with no apparent harm. (Ref) Finally, long term intakes of ~150 µg/d are supported in Japanese Natto eaters. A quick look at available Australian supplements finds doses vary from 25 -200 µg/d per capsule. (Ref)
Complicating matters you need the trans isomer form, which is the type found in food. Some vitamins contain the cis form which is not effective. (Ref) A couple of TGA listed trans MK-7 supplements are:
Vitamin K2 180mcg Supplement - 90 Tablets | ANC
Bioglan Vitamin K2 + D3 60 Capsules | Bioglan
In Japan, 45 mg/d MK-4 has been used since 1960 for osteoporosis and clinical studies have demonstrated its efficacy. (Ref) It has a short half life though and in Australia MK-7 is by far more common. (Ref, Ref)
For myself, I’m going to give natto a go. Apparently it’s beloved by the Japanese but challenging indeed for everyone else (a sort of Japanese Vegemite, if you will).
Safety
There is no record of toxicity for phylloquinone or menaquinones in humans while an animal study reported no toxicity associated with synthetic MK-7 administered at up to 2000 mg/kg or for oral administration of 10 mg/kg for 90d (that mg, not µg). The basis for this is that clotting factors are fully carboxylated (activated) in healthy people, so more vitamin K will make no difference. The exception is for patients on anticoagulant therapy, where vitamin K may interfere with anticoagulant efficacy. (Ref, Ref)
Having said this, long term high dose K2 therapy is relatively unusual, especially in western populations and it is possible, if unlikely, that some subgroups may experience deleterious effects with long-term supplement level doses.
Conclusion
It’s interesting isn’t it. Even if your not ready to add another supplement to your arsenal or try natto, may I suggest you ramp up your leafy greens? Australian vegetable intake is abysmal (Ref) and, leafy greens in particular are packed with vitamins, minerals and polyphenols while having virtually no calories. Also, FYI, it’s not a garnish, it’s half a cup cooked, or a cup raw. Got it? Next time, the final bone installment: magnesium.