
Vitamin D - the sunshine vitamin

Introduction
Vitamin D isn’t really a vitamin at all. It’s technically a hormone and it’s not a vital nutritional component either, especially not in Australia. In the last article, it came up several times as an essential partner to calcium in promoting bone health. Numerous other potential other roles for vitamin D are currently the subject of intense investigation. I don’t need to tell you the problem though: vitamin D = sun and, at least in Australia, its dangers have been most thoroughly inculcated in us. On the other hand, over 1 in 5 Australians are deficient. Yes, there are food sources and supplements too of course. But there are pros and cons to all of them. Let’s look at what vitamin D can do in the body and what might work for you. This one is pretty cool, enjoy.
Some vitamin D jargon
| Names | Other names | Other info |
|---|---|---|
| Dietary vitamin D3 | Cholecalciferol | This comes from animals |
| Dietary vitamin D2 | Ergocalciferol | This can come from yeasts and fungi |
| 25‑hydroxyvitamin D | 25(OH)D | This is the blood marker of vitamin D and I’ll call it 25(OH)D to indicate vitamin D status. |
| 1,25‑dihydroxyvitamin D | 1,25(OH)2D | This is the active form but it’s used quickly in the body so is rarely measured. |
| Minimal erythemal dose | MED | The amount of UV radiation that just causes faint skin redness |
| Parathyroid hormone | PTH | When vitamin D status is low, PTH is often high. |
| Age | Adequate Intake | Upper Limit |
|---|---|---|
| 0-1y | 5 µg (200 IU) | 25 µg (1000 IU) |
| 1-50y | 5 µg (200 IU) | 80 µg (3200 IU) |
| 51-70y | 10 µg (400 IU) | 80 µg (3200 IU) |
| 70y+ | 15 µg (600 IU) | 85 µg (3200 IU) |
IU = international units. For vitamin D 40 IU = 1 µg
Where do I get vitamin D?
Five places:
UVB rays: vitamin D3 is made when sunlight hits the skin. In the absence of supplements, this accounts for 90-95% of Australians’ vitamin D. With a lot of sun, conversion becomes saturated, so there’s no risk of vitamin D toxicity from this route, though vitamin D is pretty safe anyway. (Ref)
Dietary vitamin D3. This is generally limited. Some of the best sources are below. (Ref)
Dietary vitamin D2: Just like us, mushrooms left in the sun make vitamin D. For instance, button mushrooms generated 17.6 μg/100 g (704 IU) of vitamin D2 after 15 minutes sunbathing. D2 generation is enhanced in mushrooms with gills facing up, as well as in sliced or dried mushrooms. The vitamin is also substantially retained when the mushrooms are subsequently stored and cooked. (Ref, Ref) A caveat: vitamin D2 is less effective than vitamin D3 so 3ug of D2 might replace every 1ug of D3. (Ref)
Fortified foods: Only margarine is mandatorily fortified in Australia and voluntary fortification is also quite rare. Elsewhere, it’s becoming more common. Finland provides a good case study, where widespread fortification reduced population deficiency from 56% to 9%, without materially increasing the number of people with excessive vitamin D levels (≥125nmol/L). (Ref, Ref, Ref)
Supplements: In 2012 only 7% of the 5% of Australian adults who took Vitamin D supplements (update: 9.3% took vitamin D supplements in 2023) were deficient, compared with 23% of those who did not. (Ref) Very high supplementation, coupled with high calcium intake, can lead to accretion of calcium in the arteries, kidneys and joints and possibly other locations but this is not a risk at doses <2000 IU/d. (Ref)
| Food sources of vitamin D3 | Vitamin D (μg/100 g) |
|---|---|
| Eel | 25.6 |
| Pike-perch | 24.6 |
| Herring | 15.4 |
| Salmon | 12.4 |
| Egg yolk | 7.8 |
| Tuna | 7.2 |
| Cod | 7 |
| Egg | 2.8 |
| Beef liver | 0.8 |
| Butter | 0.3 |
We’ll come back to sunlight and supplements.
Physiology
Vitamin D from the skin or diet is taken to the liver where it is converted to 25(OH)D, the major circulating form (and what’s measured with a vitamin D blood test).
The calcaemic path
Under the influence of, principally, parathyroid hormone (PTH), 25(OH)D is converted to its active form 1,25(OH)2D in the kidneys. Activated vitamin D can then engage with vitamin D receptors (VDRs) in the small intestine to markedly increase calcium absorption, as outlined also here.
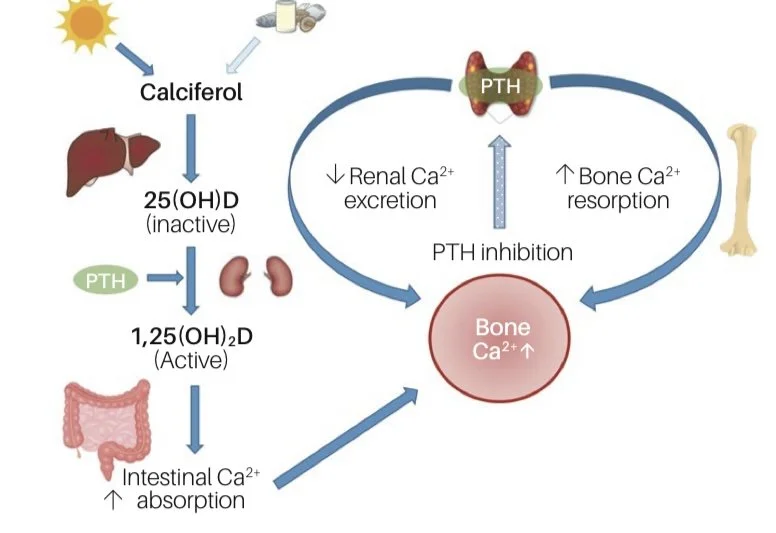
Vitamin D physiology
Source: Melbourne Pathology (2022). (Ref)
This is called the ”calcaemic path” as the purpose is to increase calcium in the blood and it’s pivotal to bone health. (Ref) Inadequate vitamin D causes rickets and osteomalacia and is also involved in osteoporosis. (Ref)
Osteomalacia doesn’t have the same profile as osteoporosis but it’s not uncommon and may co-exist with osteoporosis in severely vitamin D deficient adults. Here bone mineral is also lacking and there is also fracture risk but osteomalacia is also characterised by bone pain. It remains largely undiagnosed as diagnosis requires X-rays. (Ref, Ref)
Rickets is the childhood version of osteomalacia. Nutritional rickets is a risk in infants breastfed by vitamin D deficient mothers and in older children, particularly during the adolescent growth spurt. (Ref)
The non-calcaemic path
The enzyme that converts vitamin D to 25(OH)D in the kidneys is also found in many other cells and VDRs are also to be found throughout the body. These findings suggest vitamin D has other purposes beyond its “calcaemic” role in bone strength but, as yet, these are much less well-understood. (Ref) Some of the numerous hypothesised functions of vitamin D include reducing autoimmune disorders, cardiovascular disease, diabetes, metabolic syndrome, cancer, neurological diseases, depression, and inflammatory bowel disease.
All this sounds amazing but, while observational evidence points one way, interventional trials supplementing vitamin D have been less impressive. (Ref) There are a number of potential explanations for this conflict and it appears they may all occur to some extent! (Ref)
Reverse causation where poor health or an unhealthy lifestyle mean less time outside generating vitamin D.
Confounding, where a third factor drives both sun exposure and health. Exercise is an excellent example.
Other beneficial effects arising from sun exposure unrelated to vitamin D.
Insufficient before and after contrast in interventional trials. Ie, baseline vitamin D in interventional trials may have been too high at the outset to show benefit from supplementation.
Insufficient active arm and placebo contrast in interventional trials. As vitamin D supplementation is common in the population, the placebo group may have supplemented vitamin D during the trial creating a lack of contrast between the two groups. Instead, or as well, compliance may have been poor in the active arm.
Interventional trials of insufficient length or in the wrong cohort to show effect.
How much is enough vitamin D?
Blood serum 25(OH)D is the usual measure of vitamin D adequacy (and it’s a great help in trials to check subjects in trials are taking their supplements). Here are Australia’s cut points. (Ref)
o severe deficiency <13 nmol/L
o moderate deficiency 13–29 nmol/L
o mild deficiency 30–49 nmol/L
o adequate levels ≥50 nmol/L
o Potential adverse effects: >125 nmol/L
The Royal College of Pathologists of Australia (RCPA) advises vitamin D levels may need to be 10 to 20 nmol/L higher at the end of summer, to allow for declines over winter. You can see the seasonal variation in the chart of Melbournites below. Right now, at the end of March, vitamin D levels should be close to their annual highs.
Medicare will reimburse vitamin D testing for anyone who is at risk of vitamin D deficiency but you can also pay out of pocket for a vitamin D test.
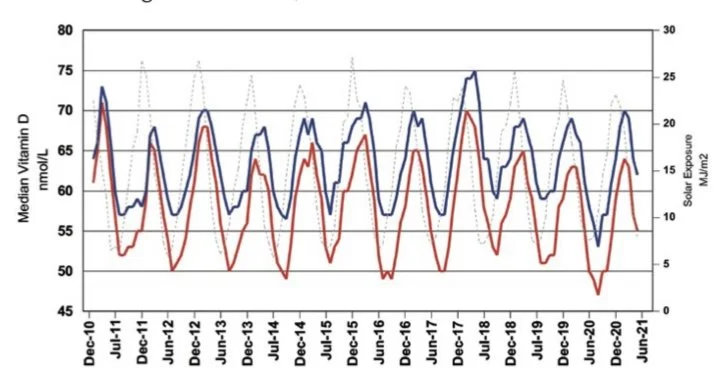
Seasonal variation in vitamin D levels in Melbourne for males (blue) and females (red) between 2010-2021. UV levels are represented by the grey dotted line.
Source: Melbourne Pathology (2022). (Ref)
Who is most at risk of vitamin D deficiency?
Lot’s of people.
Despite ample sunlight, deficiency is very common in Australia. According to the Australian Bureau of Statistics, 21% of Australians >12y were vitamin D deficient (<50nmol/L) in 2024, with young adults and men more commonly deficient. Supplementation in older adults would explain declining deficiency with age though not why men are more often lacking. As teens and young adults are still laying down bone, it’s possible that there may be greater vitamin D turnover but this looks like more of a lifestyle issue. (Ref, Ref)
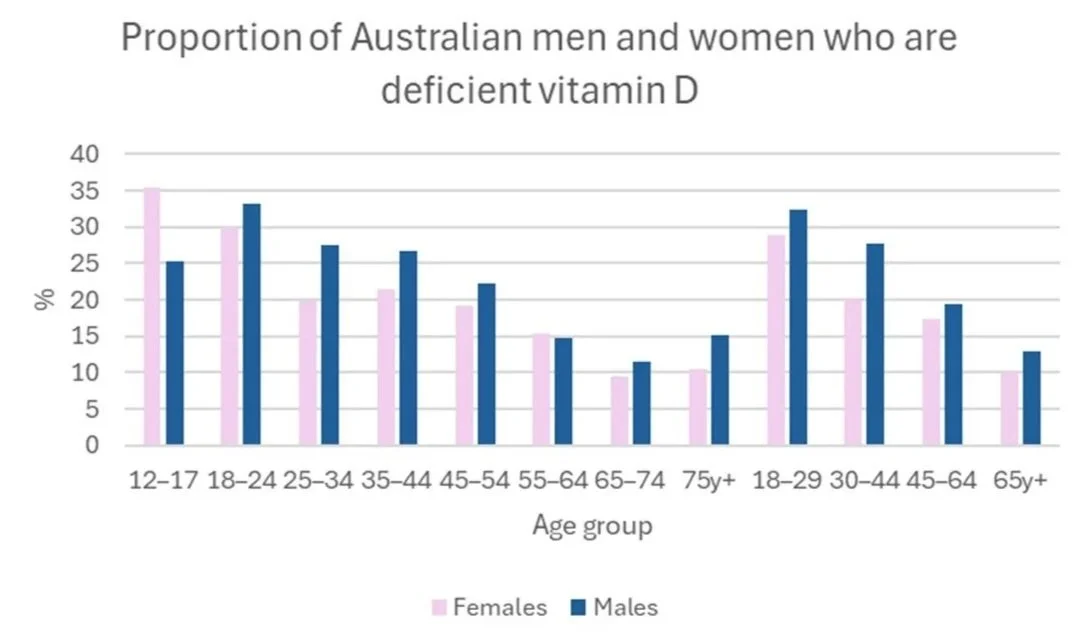
Australian Bureau of Statistics. National Health Measures Survey (2022-2024). (Ref)
Note that more men are deficient than women here but in the Melbourne chart above, men’s median levels were higher. It may be that men have more variation in vitamin D overall, such that more fall below a threshold.
People who are most at risk include:
People with dark skin. Melanin absorbs UV radiation and interferes with vitamin D synthesis.
People who cover up or who don’t go outside during the day: for obvious reasons
People living at latitudes >33°N (=Casablanca) and >33°S (=Sydney) during winter.
Babies born to vitamin D deficient mothers. (Ref) Most pregnancy multivitamins contain 400 IU vitamin D but this is not enough for women who are themselves deficient. In some cases, 1000–1600 IU/d vitamin D was still inadequate. Ideally, vitamin D should be brought up to adequacy prior to pregnancy and monitored throughout. (Ref)
Older adults, as ageing skin has reduced capacity to synthesise vitamin D; impaired kidney function reduces renal conversion to the active form; and there may also be reduced intestinal absorption of dietary vitamin D. (Ref)
Smokers: Australian ex-smokers have higher 25(OH)D than current smokers (Ref).
People carrying extra weight as vitamin D is sequestered in fat stores where it is physiologically inactive. (Ref)
Magnesium deficiency can cause reduction in the efficiency of conversion to active vitamin D. (Ref)
Diseases affecting nutrient absorption or the liver and kidneys, which interfere with vitamin D absorption and activation.(Ref)
The Sun
As we know, in Australia, the sun is both friend and foe.

Only UVB generates vitamin D but it’s also responsible for sunburn, skin cancers and cataracts. UVA can also cause sunburn, though less so, but UVA is the chief ageing agent.
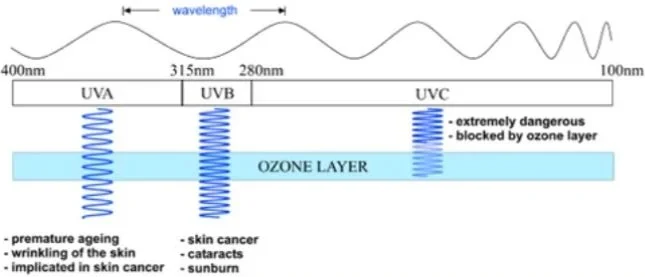
The UV spectrum.
Source: ARPANSA. (Ref)
The UV index includes UVA and UVB but it’s still a good indicator of vitamin D generating capacity. When the index is <3, vitamin D generation slows right down but it’s still possible to generate adequate amounts year-round in Sydney (if you’re willing to run around for half an hour or more in a t-shirt and shorts every day in July).
The Cancer Council's SunSmart app gives you the UV index wherever you are in the world and recommends sun protection “when the UV Index is 3 or above, or when spending extended periods of time outdoors.” (Ref) Happily, if not intuitively, most studies published to date show no association between sunscreen use and vitamin D deficiency. This is doubtless partly because of insufficient application but, even when application was rigorous, the small amounts of UV that penetrated were enough to do the job. (Ref)
Below is the average maximum UV index in Australian cities by month.
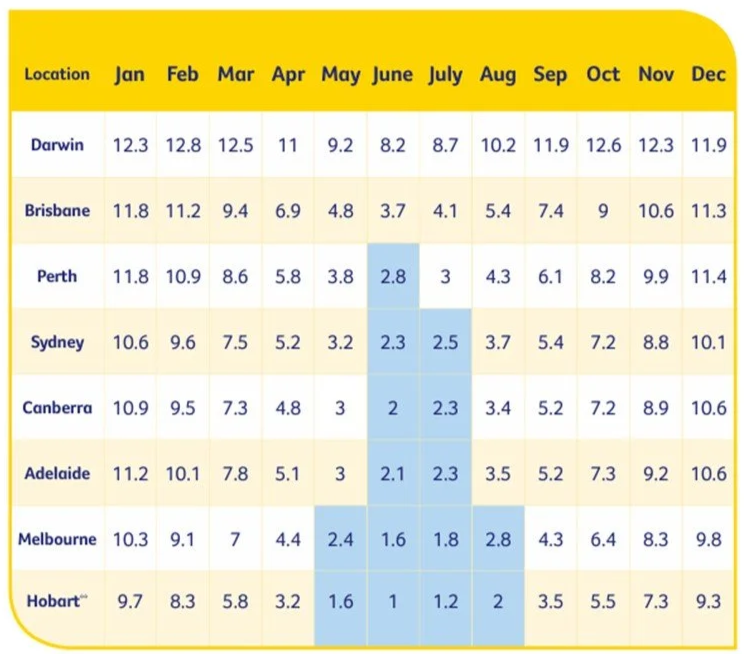
Average UV index by month in Australian cities.
Source: Cancer Council. (Ref)
And here are seasonal sun exposure minutes for adequate vitamin D synthesis on exposed arms and legs (outside the hours of 10 am – 2 pm). (Ref)
| Region | Duration (minutes) | Duration (minutes) |
|---|---|---|
| Summer | Winter | |
| Cairns | 6–7 | 9–12 |
| Townsville | 5–7 | 9–13 |
| Brisbane | 6–7 | 15–19 |
| Sydney | 6–8 | 26–28 |
| Melbourne | 6–8 | 32–52 |
| Adelaide | 5–7 | 25–38 |
| Perth | 5–6 | 20–28 |
Other than personal factors, latitude and season, clouds, smog, and glass all reduce UVB. In fact, virtually no UVB penetrates glass, though UVA certainly does. (Ref) So sitting in the window in winter will give you wrinkles but no vitamin D.
Here’s a cool and instructive tool to assess how much sun exposure you need to obtain 1000 IU of vitamin D: FastRT
Using this tool, here are my exposure minutes to generate 1000 IU of vitamin D at different times of the year in Sydney with different amounts of skin exposed. You can see the time to sunburn (MED) is the same regardless of skin exposure, so more skin is the most efficient way to get the vitamin D but not the sun damage.
| SKIN TYPE II | 10% | 25% | 50% | MED |
|---|---|---|---|---|
| SYDNEY | 1000 IU | 1000 IU | 1000 IU | |
| 21-Dec | 10 | 5 | 3 | 16 |
| 21-Mar | 16 | 7 | 4 | 25 |
| 21-Jun | 55 | 22 | 11 | 77 |
| 21-Sep | 16 | 7 | 4 | 26 |

The Fitzpatrick Skin Type Scale. (Ref)
The sun beyond vitamin D
There’s some evidence that the sun’s benefits extend beyond vitamin D and this may be one explanation as to why vitamin D supplement trials often fail to show the same benefits as might be expected based on observational evidence. It should be stressed here that this science is more speculative than that for the sun’s causal role in skin cancer but it’s an area of much scientific interest.
Firstly, higher lifetime sun exposure, as evidenced by skin damage or a history of skin cancer, is inversely associated with multiple sclerosis risk. (Ref, Ref) Evidence suggests risk is reduced both directly, by a factor other than vitamin D, but also indirectly, mediated by higher vitamin D levels. (Ref)
Blood pressure may be another example. Here, the mechanism might relate to skin stores of nitrogen oxide, which can be converted to nitric oxide by UV radiation and exported to the circulation to cause vasodilatation and reduce blood pressure. (Ref)
Supplements
To sum up: naturally occurring vitamin D3 from food is effective but hard to come by; while D2 is easy enough to produce in mushrooms but is less effective; the sun is (literally) playing with fire; and fortification is practically non existent in Australia. You can cadge together these various sources and probably get there but, since many people don’t, please welcome supplements.
Trials show that 400 IU/d and 800 IU/d of vitamin D supplementation, respectively, will achieve serum 25(OH)D concentrations of ≥25 nmol/L and ≥50 nmol/L in 97.5% of subjects. However, these trials were mostly in Caucasians (who are assisted by higher solar-sourced vitamin D) and may contain few people with excess weight (who are less responsive to vitamin D). Moreover, evidence suggests the lowest mortality risk occurs at 25(OH)D levels of about 78 nmol/L and that somewhat higher is better than lower (Ref)
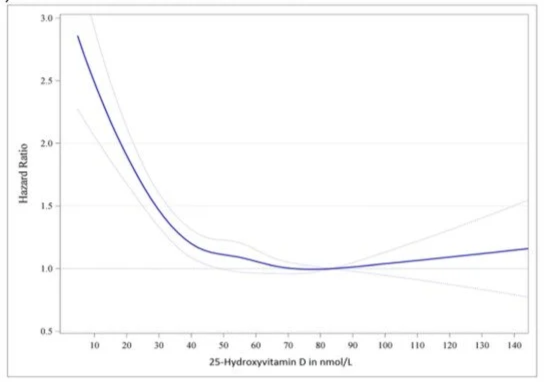
Mortality rate by 25(OH)D. Adjusted for age, sex, BMI and season. Hazard ratios (blue line with 95% confidence interval as the dotted blue lines).
Note, that reverse causation and residual confounding factors may still be present here.
Source: Pludowski et al (2024). (Ref)
Really, it’s easier to remove the guess work by testing your 12(OH)D, even if you have to pay out of pocket for it. But if you’d rather not, you can assess a couple of clinical studies as a guide to an appropriate supplement dose.
Firstly, in the VITAL trial, subjects had adequate 25(OH)D at baseline. After two years’ vitamin D supplementation of 2000 IU/d, varying levels of serum 25(OH)D were found depending on body mass index (BMI). Regardless, 25(OH)D was >80 nmol/L at all levels of BMI, while also not being excessive in any category, as shown in this table below. (Ref, Ref) This suggests 2000 IU/d is a safe and effective dose. It is however currently considered a high dose to take with a diagnosed inadequacy.
| BMI (kg/m2) | nmol/L |
|---|---|
| <25 | 110 |
| 25-30 | 103 |
| 30-35 | 98 |
| >35 | 92 |
Pludowski et al (2024). (Ref)
Secondly, the following chart from a separate study shows serum 25(OH)D increasing at a decreasing rate with supplement dose and that the effect was baked in by six months. This study was in vitamin D deficient post menopausal women (though we don’t know what subjects’ background sun exposure or dietary vitamin D intake was). Nevertheless, this might act as a guide to appropriate dosing, suggesting 1000IU/d. (Ref)
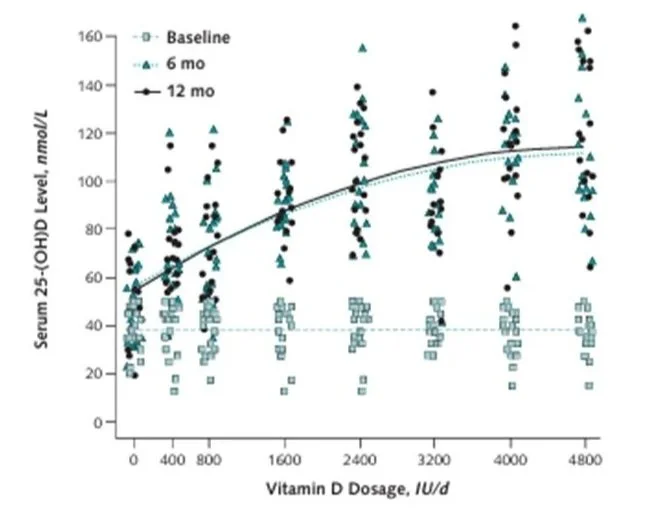
Vitamin D dose response curve. (Ref)
Without diagnosed inadequacy, 1000 IU/d is enough for the winter months if you don’t get much sun and especially if you are older, overweight or have dark skin - but in this case, your doctor should test your vitamin D as a matter of course. If you know your levels are sufficient to get you through winter, then there’s no reason to supplement at all.
One other thing, as a fat soluble vitamin, vitamin D absorption is considerably enhanced by co-digestion of fats or oils and therefore supplementation should be with a meal.
Now, let’s talk about those health benefits for vitamin D
The conundrum for vitamin D is that observational evidence supports a protective effect against numerous conditions, but proving a link with randomised controlled trials (RCTs), has proven challenging.
Bone Health
This is the most well established benefit of vitamin D.
In the last article on calcium, we saw a strong indication in observational evidence that vitamin D was more important than calcium for bone mineral density. You may remember these charts.
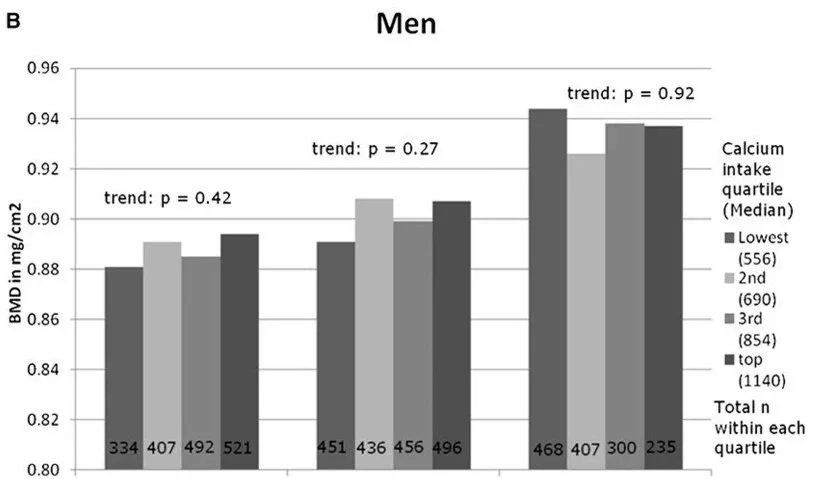
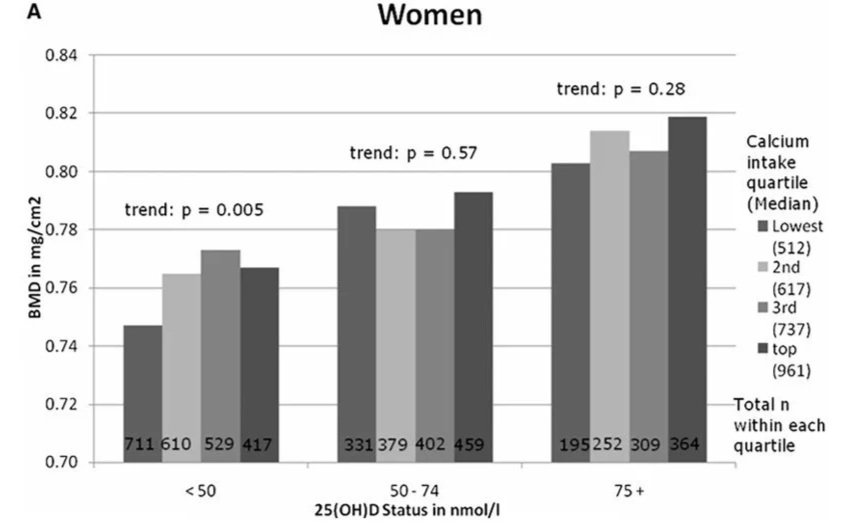
Bone mineral density by calcium intake and vitamin D status in men and women. (Ref)
Yet, in a 2021 umbrella review, it’s true calcium plus vitamin D supplementation RCTs reduced fractures, including hip fractures, in two-thirds of cases, but only in people in nursing care and not when supplementation was vitamin D alone. (Ref)
What bout muscle strength and fall risk
While improved muscle strength with vitamin D has consistently failed to materialise in anyone, whether young or old, male or female. (Ref, Ref, Ref, Ref, Ref), in adults >50y, vitamin D supplementation may modestly reduce fall risk. (Ref)
Okay so it’s a valuable member of the bone team. What about all those other conditions then?
Everything else
Cancer and cardiovascular deaths
Well, a 2014 analysis looking at both observational trials and RCTs, found solid observational evidence for the benefits of vitamin D in keeping people alive.
| Mortality risk (73 cohort studies, n = 849,412) | Increase in risk in bottom third by serum 25(OH)D compared to top third |
|---|---|
| Cardiovascular disease | 35% |
| Cancer | 14% |
| Other | 30% |
Source: Chowdhury et al. (Ref)
Note: The median baseline concentration of vitamin D in these studies was just adequate at 52nmol/L.
Unsurprisingly, studies which observed subjects for longer found greater benefits and benefits were also more marked where the use of supplements was <10% in subjects at baseline, which, the authors suggest, made for a greater contrast between the lowest and highest thirds.
Yet, the paper’s 22 included RCTs, were less compelling, despite subjects having lower baseline vitamin D (38 nmol/L) than in the observational trials. Here, Vitamin D3 RCTs found supplementation reduced mortality by 11% - though there was not enough data to tease out the causes of death that were reduced. Vitamin D2 did not show protective effects and there were increased risks of mortality in RCTs that used lower intervention doses and shorter intervention periods. (Ref)
Generally RCTs suggest that vitamin D is most helpful in reducing cancer mortality, if not incidence. The aforementioned VITamin D and OmegA-3 TriaL (VITAL) RCT, is a well-known and oft-cited RCT and the results here suggest that cancer mortality is reduced (though incidence was not, although this may be because of insufficient timeframe). (Ref)
| VITAL | Detail |
|---|---|
| Subjects | n= 25,871 US men ≥50y and women aged ≥55y. |
| Intervention | vitamin D3 (2000 IU/d), omega-3 fatty acids (1 g/d), both or none. Median duration 5.3y. |
| Results | Vitamin D did not significantly reduce cancer incidence or mortality overall, but after the first year cancer mortality reduction was significantly different to placebo to reach 25% less in the third year. |
Source: Manson et al (2019). (Ref)
In further support, a 2019 meta-analysis of 50 RCTs (n = 74, 655 subjects, average age 74y, 64% women) found Vitamin D reduced the risk of cancer death by 15%. These results were despite average trial duration <3y and the presence of very few subjects with even moderate vitamin D deficiency. (Ref) Another meta-analysis found similarly, that although vitamin D did not reduce cancer incidence overall, it did reduce cancer mortality by an average of 12%. (Ref)
And amongst cancers, the best evidence is for a reduction in colorectal cancer (CRC). Seven RCTs (n = 957 CRC cases) found a 30% reduction in adverse CRC outcomes. This included a 35% reduction in progression-free survival. (Ref)
Conclusion
There are a lot of moving parts to the vitamin D story and I expect we’ll find out more about this multi-talented “vitamin” in the coming years. As a final takeaway, low vitamin D is common, so it’s easy to be complacent, but there are clear downsides to inadequate vitamin D; it’s easy to test to find out your level; and (unlike many health interventions) it’s relatively easy to address, even if that means supplements. Next up in the bone series is vitamin K.