
Calcium - lifting the veil

Introduction
Calcium is undeniably important for bone strength but it’s not the only show in town. How much we need is contested but, in any case very few Australian adults get anywhere the recommendations. Certainly, for women at least, it’s not for want of lifelong pressure to consume more calcium. So, should we try harder? Admit defeat and supplement? Or a bit of both? This one is complex but, by the end, I hope you feel you’ve replaced your chronic low-grade calcium guilt with a plan.
Calcium in the body
Calcium’s bodily functions are numerous and include:
· Bone strength
· Heart contraction
· Muscle contraction
· Hormone secretion
· Glycogen metabolism
· Cell division
· Blood pressure regulation
· Blood coagulation (Ref)
Yes, calcium does some serious work and, in fact, bone strength is a second order priority compared to maintenance of circulating calcium within a narrow range. (Ref) The body’s levers for calcium regulation are 1) adjusting the proportion of intestinal calcium absorbed from food; 2) calibrating urinary losses; and 3) calcium sequestration in, or resorption from, bones.
Calcium in food
Below are some of the richest sources of calcium. Milk only has ~110mg/100g, but obviously serving size is ~250g, while a serving of cheese, nuts or seeds is only ~30g. Not included, but usually qualifying, are calcium fortified foods, commonly, plant based dairy alternatives (usually fortified to equivalent levels as the dairy equivalents), some breakfast cereals, some breads and calcium-set tofu. Calcium in fortified foods is generally calcium carbonate, which has equivalent absorption to milk.
| Food | Calcium (mg/100g) | Food | Calcium (mg/100g) |
|---|---|---|---|
| Poppy Seeds | 1,438 | Cooked kale | 328 |
| Parmesan | 948 | Bocconcini | 320 |
| Cheddar cheese | 760 | Fetta | 315 |
| Sardines | 725 | Liquorice | 280 |
| Mozzarella | 685 | Mycoprotein (Quorn) cooked | 274 |
| Haloumi | 620 | Almonds | 265 |
| Prawns | 583 | White chocolate | 230 |
| Chia seeds | 530 | Raw Kale | 230 |
| Camembert | 490 | Pacific Oysters | 229 |
| Whey protein powder | 420 | Rocket | 214 |
| Wattle seeds (acacia) | 419 | Firm tofu | 206 |
| Tahini | 330 | Dried figs | 200 |
| Australian RDIs | Male (mg/day) | Female (mg/day) |
|---|---|---|
| 1-3 yr | 500 | 500 |
| 4-8 yr | 700 | 700 |
| 9-11 yr | 1,000 | 1,000 |
| 12-18 yr | 1,300 | 1,300 |
| 19-50 yr | 1,000 | 1,000 |
| 51-70 yr | 1,000 | 1,300 |
| >70 yr | 1,300 | 1,300 |
| Pregnancy (adults) | 1,000 | |
| Lactation (adults) | 1,000 | |
| Upper limit (all) | 2,500 | 2,500 |
| US and Canada | Male / female (mg/day) | UK | Male / female (mg/day) | EU | Male / female (mg/day) |
|---|---|---|---|---|---|
| 1-3 yr | 700 | 1-3 yr | 350 | 1-3 yr | 450 |
| 4-8 yr | 1000 | 4-6 yr | 450 | 4-6 yr | 800 |
| 9-11 yr | 1300 | 7-10 yr | 550 | 7-10 yr | 800 |
| 12-18 yr | 1300 | 11-18 yr | 1000 / 800 | 11-18 yr | 1150 |
| 19-50 yr | 1000 | 19-50 yr | 700 | 19-25 yr | 1000 |
| 51-70 yr | 1000/1200 | >51 yr | 700 / 1200 | >25 yr | 950 |
| >70 yr | 1200 | ||||
| Pregnancy (adults) | 1000 | Pregnancy (adults) | 700 | Pregnancy (adults) | 1000 |
| Lactation (adults) | 1000 | Lactation (adults) | 1250 | Lactation (adults) | 1000 |
Regardless, Australian adults of both sexes and all ages, routinely fall well short of all calcium RDIs except the UK’s. (Ref)
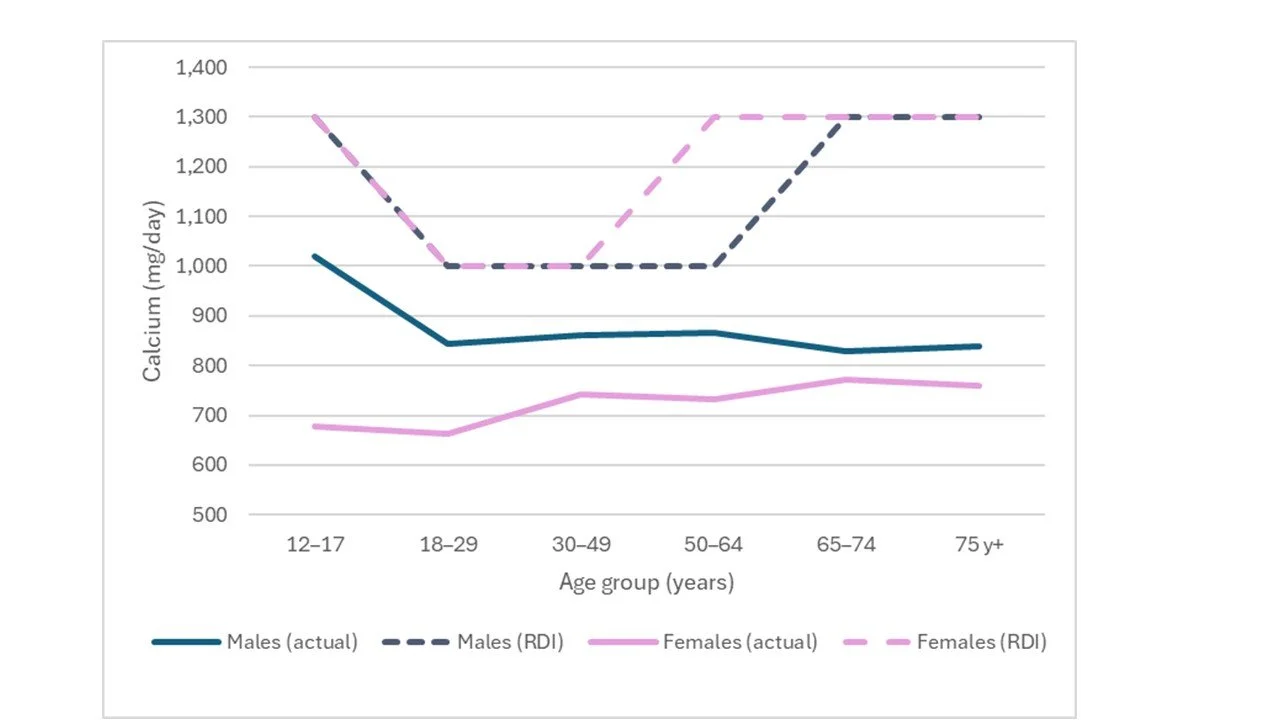
All Australian adults, regardless of sex or age fall short of the RDIs.
Much health advice advises, generally women and teen girls, to include more calcium in their diets (which in the Australian Guidelines is essentially synonymous with dairy (Ref)) and they usually include a variation on the words that it’s best to obtain calcium from your diet such as here on the Healthy Bones Australia site.
But is this new news? Is it any more helpful than earnest, repeated exhortations to women to eat more iron or new mothers to breastfeed? Perhaps it’s not a want of knowing but rather an impediment to doing? True, men may be unaware that their diets are calcium deficient, so this advice may have some effect there, but given lifelong shortfalls against the RDIs in women, the same hurdles may arise.
The Australian RDIs are now nearly 20 years old, so let’s look at the evidence in the current context.
Race
Race matters for bone strength. The chart below demonstrates a positive correlation between higher dairy (it’s not just milk) and age-adjusted fracture risk. In Western countries dairy accounts for ~70% of calcium intake but other data shows the relative country ranks are maintained when non-dairy sources are added in. (Ref, Ref, Ref)
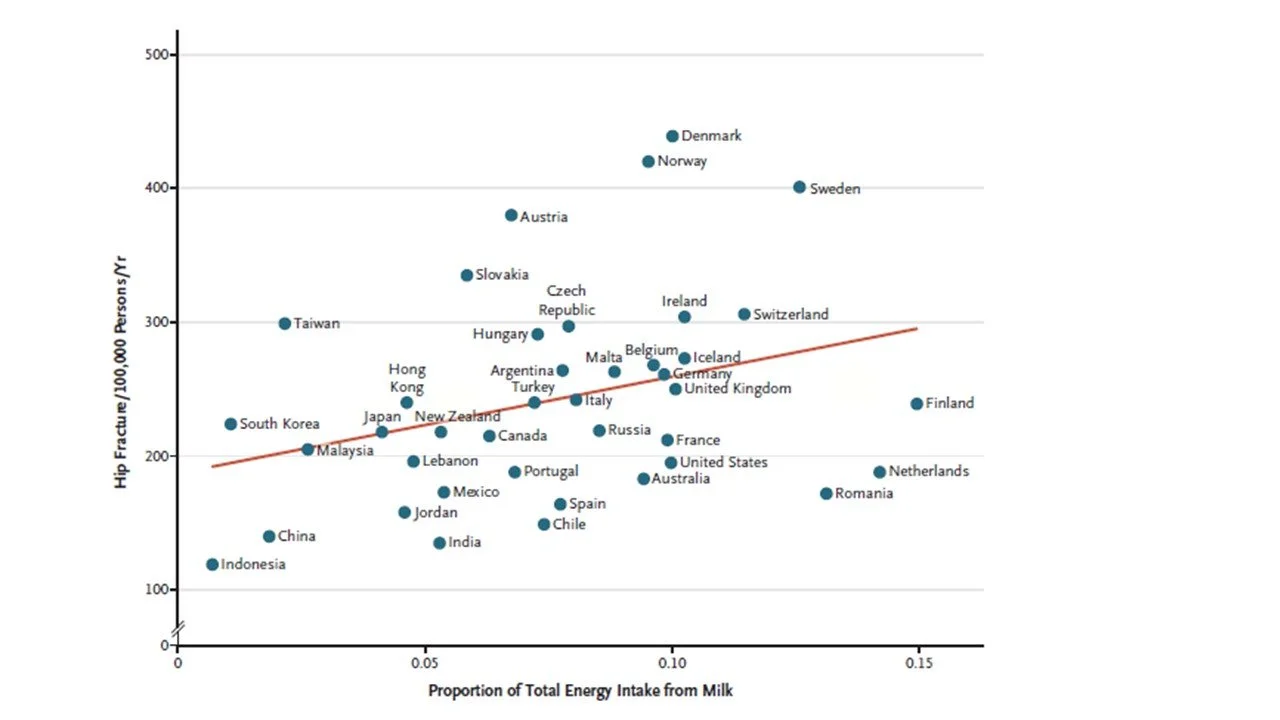
Dairy and osteoporotic fracture risk are correlated but there are other factors at play. Source: Willett et al (2020). (Ref)
However, the relationship might also be a function of race, vitamin D status, exercise, microbiome adaptations (which can augment calcium absorption) and height (big trees fall harder). (Ref, Ref, Ref)
Controlling as best we can for other variables, race is clearly a determinant with Caucasians most vulnerable. Below is the US age-standardised fracture rate per 100,000 population for women (left) and men (right).
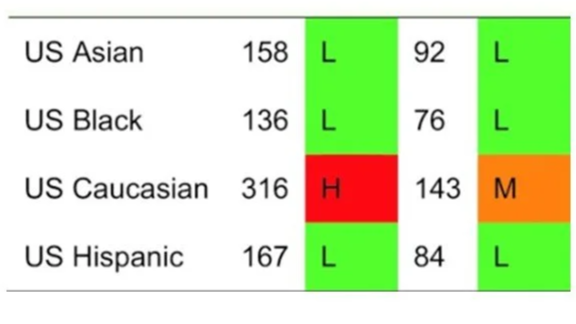
US age-standardised fracture rate per 100,000 population for women (left) and men (right). Source: Kanis et al (2020). (Ref)
So, if you’re not Caucasian does bone strength, calcium consumption and, even more specifically, dairy consumption, warrant the same focus? This is especially relevant as most non-Caucasians are lactose intolerant. (Ref)
What is the calcium balance?
While there are several approaches available, Australia’s calcium RDIs rely on calcium balance studies, where people are fed increasing amounts of calcium under jail-like conditions. (Ref)
a. Calcium intake less calcium in faeces represents net calcium absorption. About 25% absorption is average.
b. Net absorbed calcium less calcium lost in urine plus minor routes represents net calcium retention or loss.
c. Calcium balance is achieved when net retention or loss is zero. At low intakes, more is lost than absorbed, indicating a deficit, but in adults, generally there will be minimal retention and thus, once balance is reached increasing calcium intakes will see losses rise commensurately
Below, are three theoretical scenarios.
| Ca (mg/d) | % | Ca (mg/d) | % | Ca (mg/d) | % | |
|---|---|---|---|---|---|---|
| Net loss | Low intake balance | High intake balance | ||||
| Intake | 400 | 100% | 750 | 100% | 1200 | 100% |
| Faecal losses | -260 | 65% | -525 | 70% | -900 | 75% |
| Net absorption | 140 | 35% | 225 | 30% | 300 | 25% |
| Urinary loss | -140 | 35% | -195 | 26% | -270 | 23% |
| Insensible losses | -30 | 6% | -30 | 4% | -30 | 3% |
| Net gain/ loss | -30 | 0 | 0 | |||
Insensible losses are mainly sweat and don’t vary with intake. Other exit routes however do scale to intake: as intake increases, absorption falls and urinary losses rise.
The take-away is that going all-in on calcium won’t make much difference to bone mineral in either adolescents of adults. Instead RDIs aim to ensure that adequate calcium is habitually consumed so that sufficient is available for growth and bone mineralisation and, in adulthood, that your bones are never called on to replenish blood calcium.
There are a couple of competing views on calcium balance.
View 1
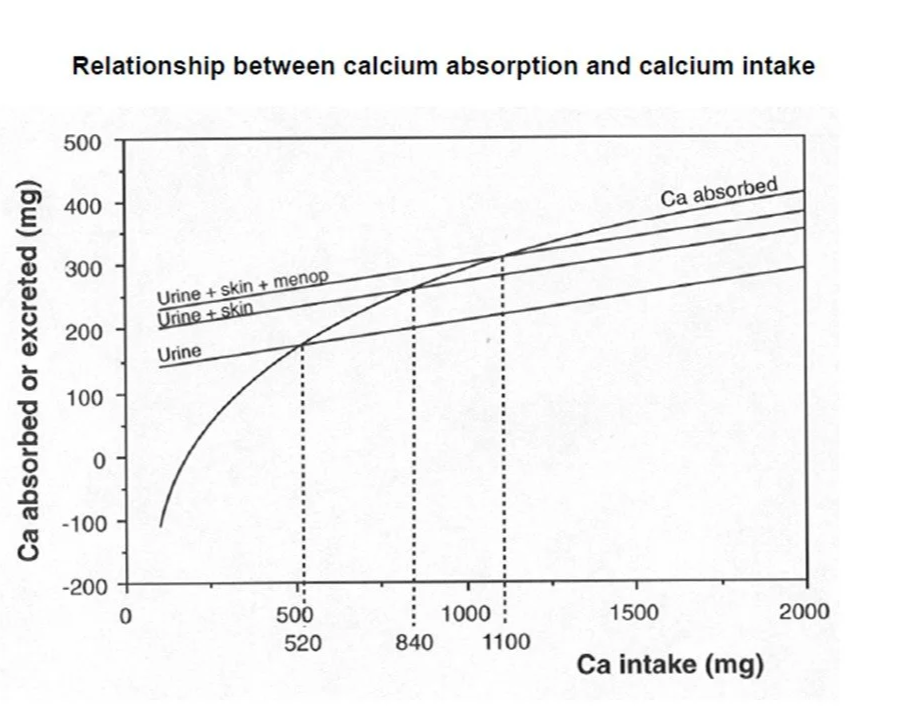
The first view comes from the World Health Organisation and the Food and the Food and Agriculture Organisation (WHO/FAO). (Ref) These estimates for adult balance (based on 210 studies in 81 subjects, averaging 90 days/study) form the basis of the Australian RDIs.
View 2
The second derives from studies, collated by Hunt and Johnson (19 balance studies in 155 subjects). This work postdates the Australian RDIs but form the basis of the European RDIs. (Ref) It’s worth reading the paper just to see what indignities these people endured in the name of science! In these studies women >50y comprised 23% of subjects (though older men were rarer) and here the age effect on calcium balance was insignificant, nor was there a sex effect.
Where the models disagreed, Hunt and Johnson, being the authors of the later set of studies, proposed reasons for the discrepancies.
Results from both studies are below. All data are in mg/day.
| WHO/ FAO | Hunt & Johnson | |||||
|---|---|---|---|---|---|---|
| Exit route | Daily loss | Absorption | Implied intake | Daily loss | Absorption | Implied intake |
| Women <50y and men | 210 | 25.00% | 840 | 186 | 24.90% | 741 |
| Women >50y | 240 | 21.80% | 1,100 | 186 | 23.30% | 798 |
Adding 2 standard deviations to cover 98% of the population, implies the intakes below, with the main difference being divergence in requirements for older men and women.
| WHO/FAO (mg/day) | Hunt and Johnson (mg/day) | |
|---|---|---|
| Women <50y | 1,000 | 1,035 |
| Women >50y | 1,300 | 1,035 |
| Men <70y | 1,000 | 1,035 |
| Men >70y | 1,300 | 1,035 |
The additional 300mg of dietary calcium in the WHO/FAO model and Australian RDIs is to cover an incremental 30mg/d increase in urinary losses in post-menopausal women. Yes, a 10% absorption rate. Why is the absorption rate so low? Absorption is the key swing factor in calcium balance, on which more below.
The WHO/FAO studies added this on to their base analysis using different studies. However, Hunt and Johnson modelled it directly (as about a quarter of their subjects were women >50y) finding calcium balance was not significantly different.
Older men are rather underserved in this area, as data is scant in both sets of studies. The Australian RDIs added the extra 300mg to men’s RDIs at 70y, by extrapolating from women.
Calcium absorption
Calcium absorption varies a lot but the body is quite able to adjust absorption to meet its needs.
Factor 1: Life stage
Babies: Human milk is low in calcium compared to cows’ milk but absorption is very high at 60%. (Ref, Ref) Post-weaning, absorption falls to ~45 % in toddlers and then ~30% by school-age.
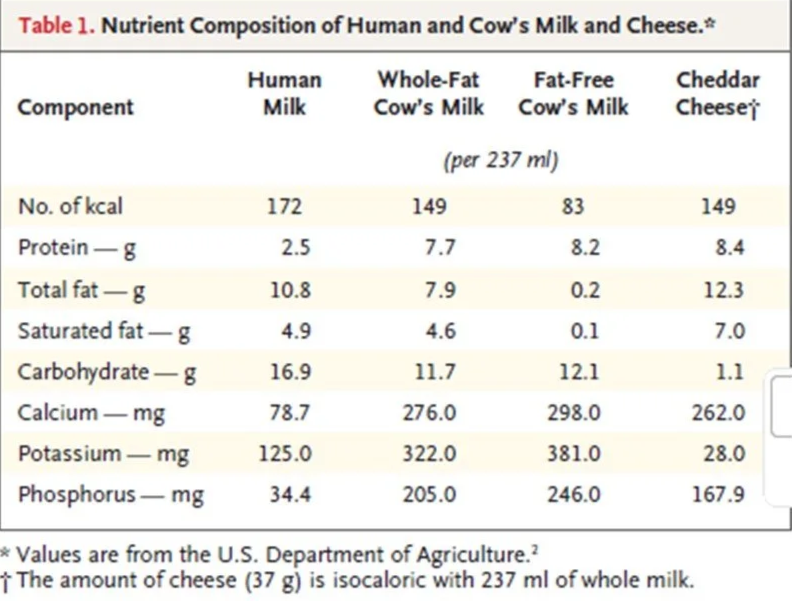
The relative nutritive value of human milk and dairy products. Source: Willett et al (2020). (Ref)
Adolescence: Both estrogen and testosterone upregulate active calcium absorption to coincide with the adolescent growth spurt. (Ref) One study found absorption in girls was 28% before, 34% during, and 25% after the early-pubertal growth spurt. (Ref) It remains at this level for some decades thereafter.
Late mid-life: In women, reduced oestrogen at menopause triggers about six years of bone loss of ~2% yearly. This loss appears obligatory and higher urinary losses and potentially lower absorption are then a secondary response to normalise blood calcium. (Ref) This would imply calcium balance should be negative at any intake, which is not the case. This is an open question in the field.
In older men lower oestrogen is also responsible for bone losses but there is no initial abrupt hormonal drop off. (Ref)
Older age: Calcium losses moderate to ~1%. Falling sex hormones may still be a factor, but reduced efficiency of vitamin D production also impedes calcium absorption. Calcium intakes also decline with overall energy consumption. At this stage blood tests may indicate elevated parathyroid hormone, a signal the body needs more calcium. (Ref)
Pregnancy and breastfeeding: During pregnancy, maternal calcium intestinal absorption doubles. While, during breastfeeding the calcium in breast milk is mostly derived from maternal bone regardless of calcium intake. At the end of breastfeeding, bone density is rapidly restored resulting in no reduction in overall density, even in teenage mothers, and there may even possibly be overall gains. (Ref) With this physiology in mind, The Australian RDIs include no extra calcium for pregnancy and breastfeeding.
Factor 2: Vitamin D
The WHO/FAO balance studies included a chart showing falling absorption at greater intakes (below). This not only occurs i) day to day, but also ii) longer term.
Source: World Health Organisation, Food and Agriculture Organisation (2002). (Ref)
This curve reflects a mix shift from vitamin-D mediated active absorption to passive absorption. While passive absorption is consistent at about 10% of intake, active absorption can be high but becomes saturated. In western populations saturation is reached at intakes ~>500mg. Hence the incremental 30mg/d WHO/FAO increment to cover menopausal urinary losses calls for an additional ~300mg intake as absorption is assumed to be entirely passive. But this is not the full story.
i) Calcium dose (day to day)
The chart below shows absorption falling with rising dose in a single meal. However, it only takes ~200 minutes for food to pass though the small intestine, where most calcium is absorbed. (Ref) And it has been demonstrated that the active transport mechanism will regenerate over several hours, such that multiple small doses will be better absorbed. (Ref) Thus, absorption can be enhanced if calcium intake is spread throughout the day. (Ref)
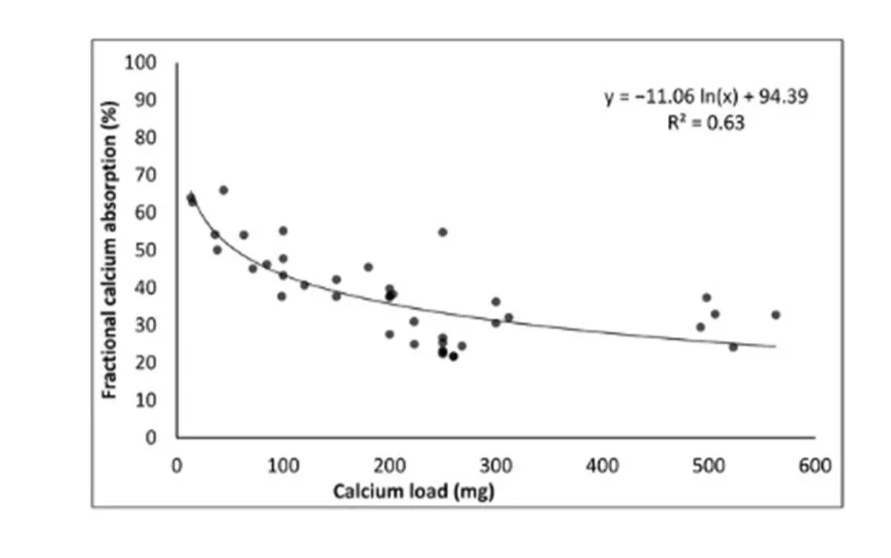
Fraction calcium absorption falls as intake increases. Source: Shkembi et al (2021). (Ref)
ii) Vitamin D receptor regulation (longer term)
When habitual intakes are low, vitamin D receptors are permanently upregulated. (Ref) In women adapted to 2,000 mg/day of dietary calcium and then switched to 300 mg/d for two weeks, absorption increased from 27 to 37%. (Ref) This may partly explain why lower intakes don’t always mean lower bone density.
Factor 3: Bioavailability
Plant based sources of calcium may be less well absorbed due phytates and oxalates, which bind calcium in the intestine hindering absorption. Cereals, legumes, oilseeds and nuts tend to be high in phytates, while spinach, rhubarb, beets, sweet potato and cocoa are classic oxalate sources. (Ref, Ref). You can see their influence on absorption in rhubarb , spinach and sweet potatoes, for instance in the chart below. However sources, such as kale and choy sum are low in oxalates and phytates hence their substantial calcium is well absorbed.
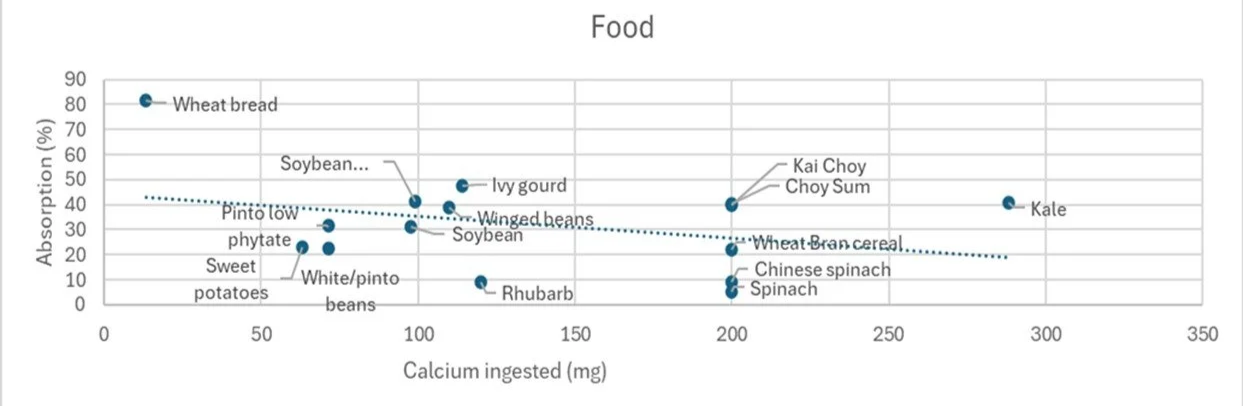
Plant sources of calcium can be well absorbed but oxalates and phytates impede efficient absorption. These are all roughly by serving size. Data source: Shkembi et al (2021). (Ref)
To lower phytates and improve calcium bioavailability: milling is effective but it also removes minerals and dietary fibre (see wheat bread above); soaking activates naturally occurring phytases which break down phytate; while fermentation entails microbial degradation of phytate as also occurs in the human colon. In fact, the colon can be a site of significant active calcium absorption if required. (Ref, Ref) Oxalates are less cooperative but boiling is effective. (Ref)
Calcium and bone health
There have now been many, many studies of the effect of calcium (very often combined with vitamin D) on bone strength. Both randomised controlled trials (RCTs) and observational population studies are numerous. These trials have also been collated into multiple systemic reviews. White women over 50y are by far the most studied and bone strength (measured by bone mineral density [BMD] and fracture rate) is invariably the issue of focus. A summary of representative trials is here.
So what does the evidence tell us?
Randomised controlled trials
RCTs point to 0-3% increase in bone density, compared to placebo, within one year of a calcium intervention. There was little indication of a greater divergence against placebo where trials continued for longer. Cessation of calcium supplementation caused BMD to revert to placebo levels. These findings applied to teens and adults of all ages and sexes.
In older adults, it appears calcium supplementation can help preserve bone but does not replace lost bone to any extent. (Ref) While most trials also supplemented vitamin D, a lesser effect was still apparent with calcium alone. There was no convincing indication that this translated into reduced fracture risk, though this may have been a function of too short a timeframe.
Where supplements appear most beneficial (though maybe this is down to compliance) is in the very elderly in care homes, where calcium combined with vitamin D can compensate for low intake and poor absorption.
There was no clear signal for optimal dose and both supplements and food-based interventions were equivalent.
Compliance was a common problem in trials and results were often adjusted to exclude non-compliers. However, as there is no reliable biomarker for calcium in the blood, accurate exclusion relies on participant honesty. Thus, the effects of calcium intervention may be understated.
Observational studies
Observational population cohort studies help colour in the picture. Here there was a stronger indication that low calcium intakes (here we can assume they were long-term and habitual) were significantly associated with weaker bones in women but only at the lowest quartile of intake (<750mg/d). In addition, where it was assessed, bone density was only lower when both serum vitamin D was low and calcium intakes were in the lowest quartile. (see chart ‘A’ below) Above this level there was no statistically significant benefit from higher calcium in women, regardless of age. Calcium intake had no link to bone strength in men at any level of intake, regardless of vitamin D status, though the lowest intakes in men were higher than those of women. (see chart ‘B’ below) Vitamin D status appears a more important determinant of bone strength.
While above the lowest quartile there was no statistical significance between intakes, a Swedish study in 61,433 post-menopausal women found a trend for fracture risk to fall with increasing intakes up to about 950mg/d, see third figure below.
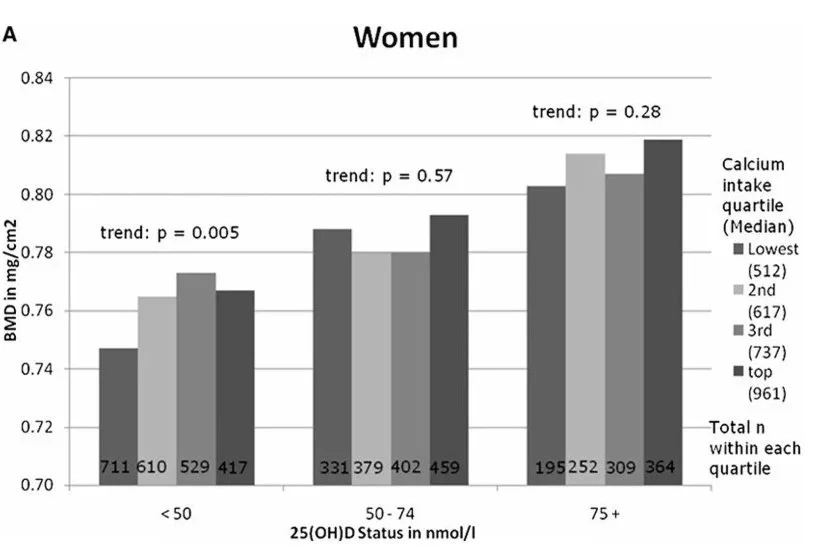
US NHANES study in 10,000 adults. Women’s total hip BMD by calcium intake categorised by serum vitamin D status. (A) quartiles: lowest <566 mg/d; second = 567–671 mg/d; third = 672–825 mg/d; top = 826–2143. Controlling for calcium intake, age (10-yr age categories), race/ethnicity (white, black, Mexican American), body mass index, height, total calorie intake, estrogen use among women, physical activity, smoking, and socio-economic status. These relationships held this relationship held regardless of age group.
Source: Bischoff-Ferrari et al (2009). (Ref)
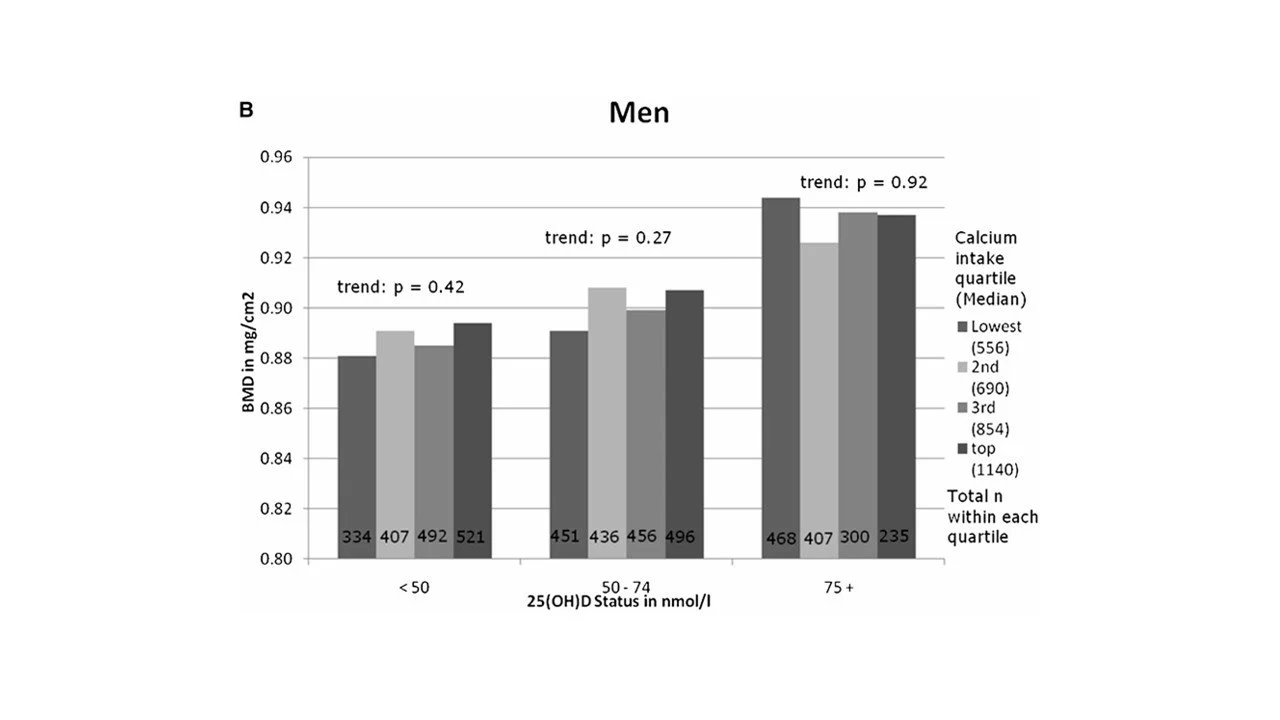
US NHANES study in 10,000 adults. Men’s total hip BMD by calcium intake categorised by serum vitamin D status. (B) quartiles: <lowest 626 mg/d; second = 627–761 mg/d; third = 762–962 mg/d; top = 963–2152 mg/d. Controlling for calcium intake, age (10-yr age categories), race/ethnicity (white, black, Mexican Amer ican), body mass index, height, total calorie intake, physical activity, smoking, and socio economic status.These relationships held this relationship held regardless of age group.
Source: Bischoff-Ferrari et al (2009). (Ref)
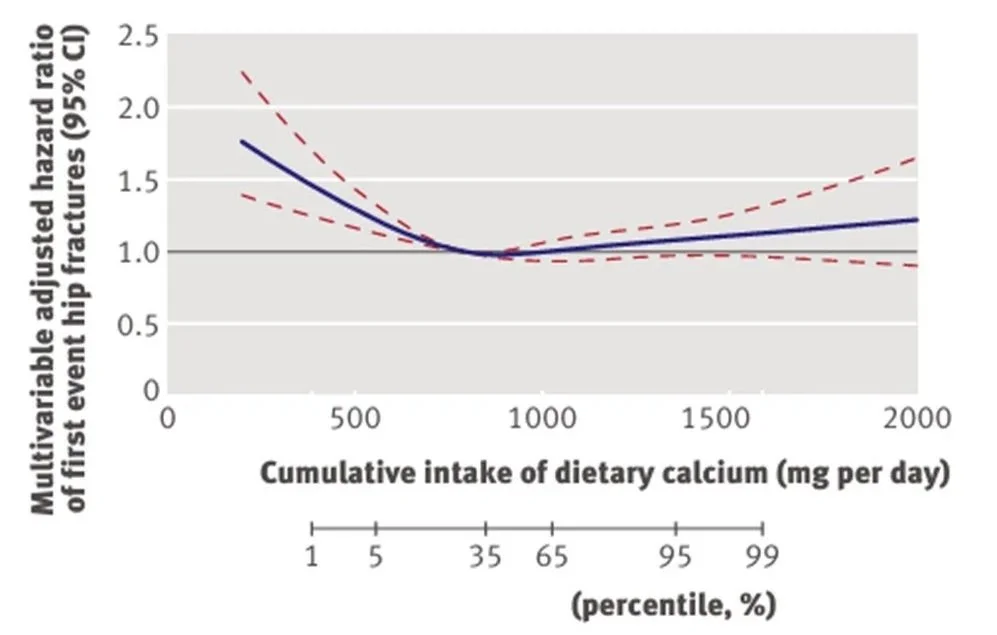
The relationship between daily calcium intake and the rate of first hip fractures from the Chart from the Swedish Mammography Cohort Study, which assessed fracture rate compared to calcium intake after 19 years. Here, the lowest point for fracture was at about 950 mg/d. The uptrend at higher intakes is not statistically significant as the red dotted line crosses zero.
Source: Warensjo et al (2011). (Ref)
Takeaway 1: Based on this evidence 1000mg a day is sufficient in adults of both sexes and all ages.
Supplementation
If your intake is average and hovers around 750mg/d, then a single glass of milk, or fortified equivalent, or 100g of kale will get you to 1000mg. But, if you’re not feeling it, is a modest level of supplementation expedient?
Supplements are usually calcium carbonate or calcium citrate and are roughly equivalently absorbed and to a similar degree as dairy. The exception is people with low stomach acid (and this is many older adults), where calcium citrate is better absorbed. Moreover, it is equally well absorbed with or without food, whereas calcium carbonate absorption is better with a low calcium meal. (Ref, Ref)
Takeaway 2: Calcium citrate is a better choice as it is not dependent on stomach acid.
Can you get too much?
When the dietary guidelines include an upper limit, in Australia’s case 2500mg/d, then the answer is yes. Though new evidence suggests 1,400mg/d is more appropriate.
Iron Absorption
Declining absorption with high intake make calcium relatively harmless. However, in the intestine, high calcium concentration can interfere with iron absorption and cause constipation (Ref, Ref)
Ectopic calcium
However, it’s not quite true that calcium is benign. One study found 9% of women taking calcium supplements had hypercalcemia (high blood calcium) and 31% had hypercalcuria (high urinary calcium) indicating too much was being absorbed. (Ref) What’s the harm? Excess calcium pumped through the body can be deposited in places other than bone, for instance the arteries, joints, kidneys and possibly elsewhere. (Ref)
Kidney Stones
The incidence of nephrolithiasis is about 10% in developed countries, with most stones composed of calcium oxalate. It’s commonly believed that higher dietary calcium increases kidney stone risk as more will be absorbed in absolute terms and therefore more will be eliminated in the kidneys. However, in fact higher dietary calcium protects against kidney stones, perhaps as it chelates oxalate in the intestine. (Ref, Ref)
There is however some suggestion that vitamin D might increase absorption and therefore urinary excretion. This is especially the case for supplements taken between meals and thus without dietary oxalates. (Ref, Ref)
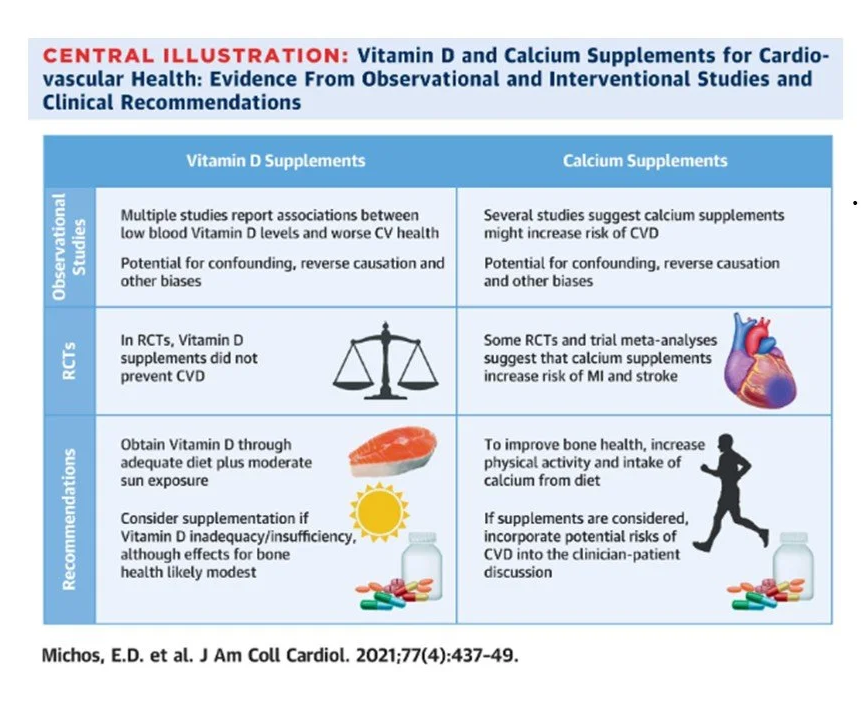
Heart disease
Concerns about heart disease and high calcium intake have ebbed and flowed for some years. And again, the Swedish Mammography cohort is instructive (only women, obviously, but regreattably). Compared with intakes of 600-1000 mg/day, intakes >1,400 mg/day were associated with 40% higher death rates overall, driven by deaths from cardiovascular disease, which were 49% higher. Calcium supplementation of 500mg/d was not associated with harm as long as it didn’t contribute to intake >1400 mg/day. (Ref)
What’s happening here? A number of factors may be at play. High blood calcium causes short term blood pressure spikes and increased propensity for blood to coagulate. Longer term, arterial calcification causes arterial stiffnes and may cause plaque instability. (Ref, Ref)
Conclusion: Aiming for 1000mg/day is sufficient. Ideally this would come from food but supplementing with up to 500mg/d calcium citrate to achieve this level is unlikely to cause harm. To minimise spikes in blood calcium and the risk of adverse effects, supplement with food and ensure your hydration is maintained.
Finally: Remember calcium is only one player and your bones have no incentive to gain mineral if they never get used! Next up vitamin D.