
The Lancet’s 14 risk factors for Dementia

Building cognitive reserve is protective throughout life.
Introduction
Friends, I’ll come back to calcium soon because I wanted to make a quick detour to bring your attention to the 2024 update from the Lancet Commission on Dementia, which was last updated in 2010. The good people at The Lancet have made it free to the public and you can read the report in full here.
Background
Dementia is now Australia’s leading cause of death. (Ref) But dementia is not genetically predetermined, nor is it mostly just bad luck. Modifiable risk factors play a major role and the Lancet Commission has identified 14 factors that the authors suggest account for about half the burden from the disease. The commission hopes that by raising awareness of these risks, they can addressed directly.
Just a quick definition: Dementia is an umbrella term for many underlying conditions that result is similar symptoms. Alzheimer's disease is often used synonymously with dementia and is the cause of about 70% of dementias. Other common forms include vascular dementia, secondary to heart disease or stroke, and Lewy bodies dementia. (Ref)
Back to the report: The degree of risk from each factor tends to increase with duration and severity. For example, with high blood pressure, both the years of blood pressure elevation and the degree of elevation, both add to the risk. So, addressing modifiable risk factors early and rigorously is desirable.
Here, the Lancet report makes clear, pharmaceuticals have been most tested and in many cases are very effective. Lifestyle interventions can’t compete, however they can address multiple risk factors simultaneously; generally come without adverse side effects; can mitigate a risk factor before it becomes overt; and are within your power to instigate. Thus, lifestyle interventions may reduce the need for medical therapies if adopted earlier in life; while they complement medical therapies when required.
What are the factors then?
Okay, that’s enough what are these factors?
| Risk Factor | Time of life when risk factor has the most effect | Percentage reduction in dementia cases if this risk factor is eliminated |
|---|---|---|
| Less education | Early-life | 5% |
| Hearing loss | Mid-life | 7% |
| High LDL cholesterol | Mid-life | 7% |
| Depression | Mid-life | 3% |
| Traumatic brain injury | Mid-life | 3% |
| Physical inactivity | Mid-life | 2% |
| Type 2 diabetes | Mid-life | 2% |
| Smoking | Mid-life | 2% |
| Hypertension | Mid-life | 2% |
| Obesity | Mid-life | 1% |
| Excess alcohol | Mid-life | 1% |
| Social isolation | Later-life | 5% |
| Air pollution | Later-life | 3% |
| Vision loss | Later-life | 2% |
Source: Livingston et al (2024). (Ref)
Hearing loss and high low density lipoprotein (LDL) cholesterol are new to this report and in future iterations it’s probable that other factors will be added.
The table from the report (below) suggests that the 14 factors share common underlying mechanisms.
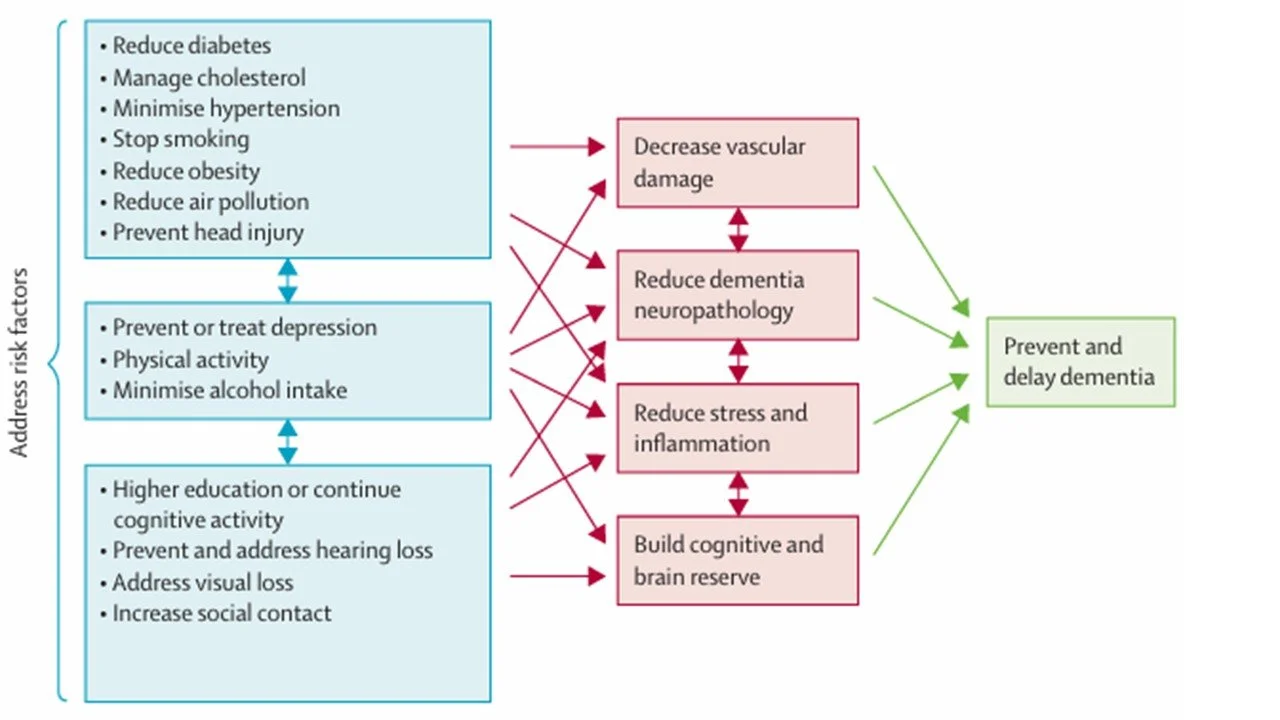
Common mechanisms link dementia risk factors.
Source: Livingston et al (2024). (Ref)
Where does nutrition come in?
From these 14 factors, High LDL cholesterol, Diabetes, Hypertension, Obesity and Excess alcohol are within the purview of nutrition. Nutrition can also modify depression and exercise is ineluctably joined with nutrition as part of lifestyle management.
The report found that management of LDL-C, diabetes and hypertension through medication mitigated dementia risk. There was no data on GLP-1 receptor agonists for obesity but they were effective for diabetes and there is no reason to suppose they won’t reduce the link between obesity and dementia also. In the spirit of addressing risk factors rigorously the evidence points to medication as the most effective measure.
But perhaps you want to do better; maybe the side effects are intolerable; or perhaps you are in that grey zone where you don’t qualify for medication but your test results are suboptimal? Also, many of these risk factors are fellow travelers so there’s a multi-bird per stone effect.
The report suggests that dietary patterns, specifically the Mediterranean diet may be helpful in managing wholistic risk. Unlike medications, dietary patterns don’t lend themselves readily to randomised controlled trials. However, the PREvención con DIeta MEDiterránea (Predimed) trial was indeed a dietary RCT which tested the Mediterranean diet (either with olive oil or nuts) against a conventional low fat diet* over four-years as an intervention to manage heart disease. Predimed found that The Mediterranean diet (both olive oil and nuts) improved cardiovascular markers, including blood pressure, LDL-C and inflammation which also translated into lower incidence of cardiovascular events. (see chart below)(Ref) It also reduced new diabetes cases (Ref); and waist circumference was lower, though in the Mediterranean + nuts group only. (Ref) Also, only in the Mediterranean + nuts group there was an improvement in depression. (Ref) Finally, while not equivalent to dementia, cognition scores were higher in those allocated to the Mediterranean diet. (Ref) So we can draw a direct line between the Mediterranean diet and dementia risk factors, even if a link to dementia itself has not be conclusively tested.
*it must be acknowledged that the low-fat group did not end up lowering their fat intake much at all so this was more of a ‘business-as-usual’ diet.
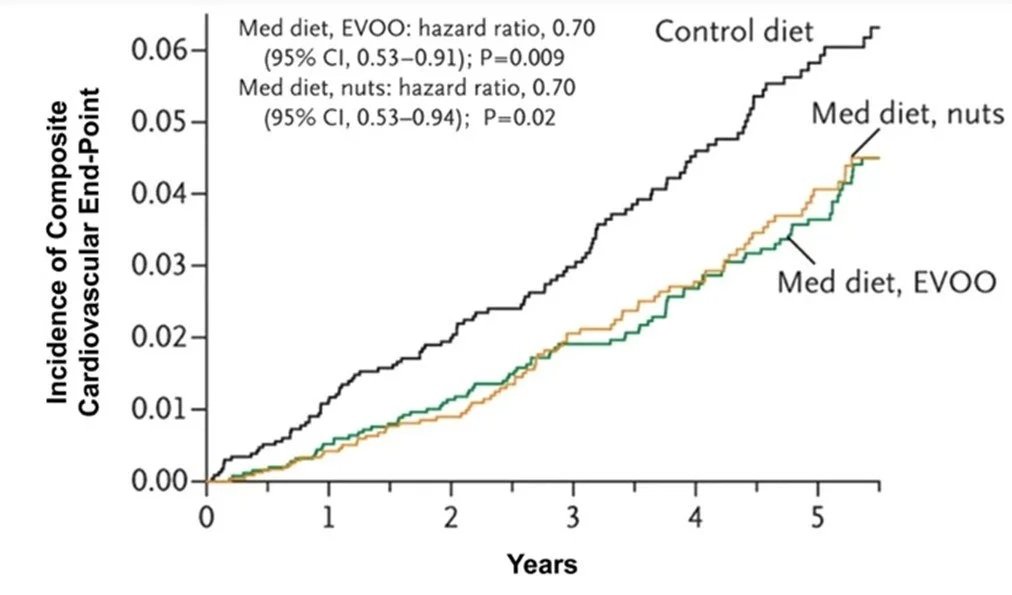
The composite cardiovascular measure includes myocardial infarction, stroke, and death from cardiovascular causes.
Source: Estruch et al (2013). (Ref)
Beyond the Mediterranean diet, there is the Dietary Approaches to Stop Hypertension (DASH) diet designed to lower blood pressure; (Ref) The Mediterranean-Dietary Approach to Systolic Hypertension (DASH) diet intervention for neurodegenerative delay (MIND) which has generated some positive evidence for cognitive preservation (the purpose for which it was initially designed) and also appears supportive in mitigating depression; (Ref, Ref) and the Portfolio diet which targets LDL-C and has demonstrated its effectiveness in cohort studies. (Ref, Ref) These diets are actually all dietary patterns and all extensions of the Mediterranean diet with emphasis on particular foods which are more relevant to the condition at hand.
I think we all more or less know what the Mediterranean diet is by now. Just in case you missed the zeitgeist its heavy on fruit, vegetables, legumes and minimally-refined grains. Fats come from extra virgin olive oil, nuts and seeds as well as fatty fish; dairy is generally fermented as yoghurt and some cheese; and red wine is usually included too. You may not also be aware that an emphasis on locally-grown seasonal produce and socialising at mealtimes are also considered key elements. It is also increasingly accepted that the Mediterranean diet could be substituted with any local version of a plant heavy-diet where processing is minimal and saturated fat, added sugar and salt are also kept low. (Ref)
There is much to like in the wholistic dietary pattern approach. It’s flexible and marketable and doesn’t get too tied up in the detail. Certainly, it’s a paradigm which has been embraced with prodigious passion by the nutrition fraternity, so much so that other perspectives are now rather unwelcome. The problem though is that, humans being humans, there is a temptation to emphasise the fun things (Olive oil! Cheese! Red wine!) and forget about those less-glamorous workhorses like vegetables and legumes, yet retain the vibe that you’re sticking to a healthy eating pattern. I’m not saying this is you but it would be easy to do…
Conclusion
Cardiovascular disease, diabetes, obesity and exercise are all major topics in nutrition and there’s much more to say. For now, this is simply a caution against complacency. Yes, high blood pressure, a few extra kilos etc are very common but they’re also manageable and future you will thank me.